

Abstract
Spasticity is a frequent symptom in people with Multiple Sclerosis. Whilst many respond to first-line therapies it is estimated that 30-40% will have suboptimal treatment response requiring more specialised management. Such strategies include combination of oral medications, botulinum toxin, nabiximols and consideration of intrathecal therapies; baclofen or phenol. Early expert intervention as outlined in this review can have a positive impact on functional ability and quality of life for people with MS.
Multiple sclerosis (MS) is one of the leading causes of non-traumatic acquired disability in young people affecting more than 120,000 people in the UK and about 2.5 million people worldwide [1]. Significant advances have been made in MS disease-modifying therapies (DMTs) including the progressive phase [2]. However, many people live with troublesome symptoms related to the disease. The North American Research Committee on MS (NARCOMS) Registry has identified 11 key symptom domains that are commonly affected in MS: mobility, hand function, tremor/coordination, vision, pain, fatigue, bowel/bladder function, sensory, spasticity, cognition, and depression [3]. More than 80% of respondents reported spasticity during their disease course and spasticity severity was reported as moderate or high by between 35% and 54% of respondents. This was associated with stiffness, spasms, and/or pain, mainly in the lower limbs. Key aspects of managing MS-related spasticity are understanding the pathophysiology of spasticity, the use of appropriate outcome measures, and a personalised approach to pharmacological treatment in the context of the patient’s activities and quality of life.
Spasticity is defined by Lance as “a motor disorder characterised by a velocity-dependent increase in tonic stretch reflexes with exaggerated tendon jerks, resulting from hyperexcitability of the stretch reflex, as one component of the Upper Motor Neuron Syndrome”. It is clinically important to differentiate between neural and non-neural components of stiffness to inform management. Optimum management requires a multidisciplinary team approach including a Neurologist or Rehabilitation Medicine Physician, Physiotherapist, Specialist Nurse, and access to occupational therapy and splinting.
Assessment and outcome measures
A thorough assessment of the impact of spasticity on the individual is key. This involves accurate history taking as to the symptoms the individual experiences, diurnal variation, trigger factors including infections, bladder and bowel dysfunction, skin breakdown, suitability and fit of splints, and impact on walking and other activities. Generic and disease-specific outcome measures can be used. A combination of objective (hands-on) and patient-reported outcome measures is essential to understand the degree of spasticity experienced and to monitor response to any intervention. The most commonly used measure is the Ashworth or modified Ashworth scales which are easy to administer in clinical practice [4]. There are conflicting reports, however, regarding the validity and reliability of these measures. The Tardieu scale, commonly used in cerebral palsy and stroke, has not been validated for use in MS spasticity [5]. The MS spasticity scale (MSSS-88) is an 88 item patient-based interval level scale that evaluates the symptoms the patient experiences and how spasticity affects their daily life [6]. The numerical rating scale for spasticity (NRS) is a 0-10 point scale where the individual will rate the severity of their spasticity over the previous 24 hours [7]. There is a concern, however, that the individual might rate other symptoms such as weakness or pain, rather than spasticity in isolation, however, this may additionally reflect the quality of life. Other measures which might be useful in clinical practice include a spasm score or functional measures such as timed walking tests (25 foot walk, 10 metre walk) or measures of upper limb function (9 hole peg test).
Current pharmacological treatments
The basis of pharmacological treatment of MS spasticity remains with the use of first-line agents: Baclofen, Tizanidine, and Gabapentin (pregabalin) [8]. Whilst many will respond to such treatment about one-third will continue to experience problematic symptoms [9]. The addition of second-line agents such as benzodiazepines (e.g. diazepam and clonazepam) may be helpful but are frequently associated with side effects including CNS depression, memory impairment is common as is dependence and withdrawal syndrome if stopped abruptly. Although there are distinct mechanisms of action, many of these agents may serve to hypopolarise neurons, such as through opening of chloride channels (benzodiazepines) or potassium channels and blockage of calcium channels (baclofen and cannabinoids), to block hyperexcitability, to quell the spastic response [10]. Dantrolene is unique in its mode of action impacting the contractile mechanism of skeletal muscle by decreasing the release of calcium. Its use is limited by frequent side effects including gastrointestinal symptoms, weakness, sedation, and dizziness. The risk of hepatotoxicity is a major limiting factor and requires monitoring of liver function prior to and during therapy. In a Cochrane review of anti-spasticity agents for MS the conclusions were that there was in general low-quality evidence of the efficacy of these agents to treat MS-related spasticity and that better outcome measures are required in trials to reflect efficacy and impact on quality of life [11].
Cannabinoids and MS spasticity
Cannabis has been used recreationally and medicinally by people with MS for many years prompting a research programme investigating the utility of cannabis-based medicinal products (CBMPs) in MS [12-14]. Biologically there is evidence that cannabis-based products modulate spasticity via CB1 receptors [15]. The whole plant extract contains hundreds of chemical entities, however, the two components of greatest interest are delta [9] tetrahydrocannabinol (THC) and cannabidiol (CBD) as the major psyochactive and non-psychoactive ingredients of cannabis that has been recently approved for some epilepsy conditions, respectively. Studies investigating synthetic THC, whole-plant extracts, smoked cannabis, and THC:CBD (Nabiximols) have been reported [12,16-18]. In 2010 THC:CBD (Nabiximols) was licensed for moderate to severe MS-related spasticity having shown a significant improvement in patient-reported spasticity on the NRS as compared with placebo [18]. In this pivotal trial, the patient cohort was enriched only randomising responders to ongoing treatment or placebo. The use of an enriched design is controversial as is the NRS spasticity as the primary outcome, thus many regulatory bodies do not accept this as high-quality evidence, despite some positive evidence of effects on the Ashworth scale in small-scale academic studies [19-20]. However, currently THC:CBD is unlicensed by the Food and Drug Administration (FDA) and variably reimbursed throughout Europe. In the UK, NICE MS clinical guidelines have recommended against its use as it is not deemed cost-effective [NICE MS CG 186 2014]. Cannabis-based products are also available in North America, Australia and in some European countries, and in November 2018 cannabis-based products for medicinal use were moved to Schedule 2 of the Misuse of Drugs Regulations 2001 raising the profile and demand for CBMPs. Many people with MS are using CBD or whole plant products, however, there is a lack of clinical trial evidence that these treatments are effective and there has yet to become a recognised supply route for medical practitioners [21].
Botulinum toxin
BoNT mediates its effect by interfering intracellularly with the process of Ca2+ regulated synaptic vesicle exocytosis, and thereby preventing the release of their contents into the synaptic cleft, namely acetylcholine [22]. Early trials of BoNT in MS addressed hip adductor tone and showed a significant reduction in spasticity and an improvement in passive function, particularly perineal hygiene. It should be considered as a useful option for focal problem areas and avoids the central side effects of systemic agents. A recent consensus group has published the UK National guidelines on use of botulinum toxin in the management of adult spasticity http://www.rcplondon.ac.uk [23].
Intrathecal Baclofen
Intrathecal baclofen (ITB) is administered via a programmable, subcutaneously implanted drug delivery system, delivering low doses of Baclofen directly intradurally around the spinal cord where GABA-B receptors are expressed in high density. It should be considered in people with predominantly lower limb spasticity inadequately managed by 1st and 2nd line oral agents. In our experience reporting the impact of ITB in 106 people with MS, the benefit of ITB has proved to be sustainable over time with a positive impact on the Ashworth scale, spasm scores, and range of movement and has the added benefit of withdrawing oral medications and reduced side effects [24]. Early series concentrated on people with significant levels of disability but more recently ITB proved to be effective in improving mobility in carefully selected individuals; prompting ITB to be considered earlier to improve or maintain walking [25]. The main concern in ambulatory individuals is that the therapeutic effect may increase weakness and negatively impact on walking and transfers, as some people with MS are reliant on a degree of hypertonia to be able to transfer and mobilise. In our cohort at the NHNN we have found that preserved baseline walking speed and lower limb muscle strength predict ambulation after ITB25 {Sammaraiee, 2019 3287 /id}. In another recently published cohort following 47 subjects for up to one year, 32 remained ambulatory for up to one year. Efficacy was also noted on modified Ashworth, NRS pain and spasm [27].
Chemical Neurolysis
Chemical neurolysis consists of either a local injection of ethanol or phenol to manage an area of focal spasticity or when administered intrathecally for severe lower limb spasticity in people not appropriate for ITB. As a focal treatment, it may act as a substitute for BoNT if repeated injections are considered detrimental to the patient or not considered cost-effective. This topic has previously been reviewed in ACNR [28] {Gaid M, 2012 3291 /id}. Phenol or alcohol mediate their effect through two different pathways, low dose eg 2% phenol for an anaesthetic effect or high dose eg >3% phenol for neurolysis causing denaturation and fibrosis of the nerve which is largely irreversible [29]. Similarly, low dose alcohol has an anaesthetic effect and high dose (>50%) is neurolytic. Following phenol treatment, partial nerve regeneration and sprouting occur so that the clinical effect may ‘wear off’ in about 30%. In our experience, intrathecal phenol is a highly effective treatment in carefully selected subjects. It will usually impair bowel, bladder and sexual function and management plans must be in place in this regard. At the NHNN over a 12 year period 2006-2018, 45 people underwent ITP successfully with a reduction in spasticity on the Ashworth scale, penn spasm scale and higher levels of comfort. Due to its destructive and potentially irreversible nature ITP remains a last resort.
Discussion
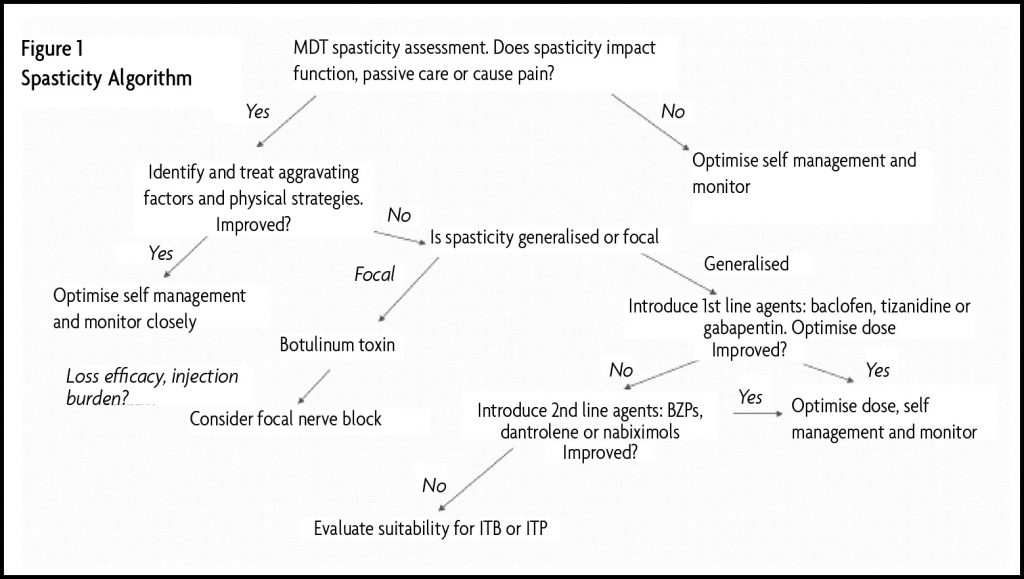
Spasticity remains a problematic symptom in people with advanced MS and when sub-optimally treated leads to significant impairment and distress. Unlike the DMT options for MS there are limited new drugs for spasticity, nabiximols being the only recently licensed option, with severely restricted access. People with MS should be treated with at least two first-line agents commencing at low doses and escalating the dose frequently until the effect is gained, side effects appear or the maximum dose is reached. Second-line agents should then be added for additional effect. Botulinum toxin or focal nerve blocks are useful for localised problematic areas. In people, including those who remain ambulatory, who have failed 1st and 2nd line systemic agents, intrathecal therapies are reasonable options and they should be referred to specialised multidisciplinary service for optimal management.
References
- Compston A, Coles A. Multiple sclerosis. Lancet 2002;359(9313):1221-1231. https://doi.org/10.1016/S0140-6736(02)08220-X
- Montalban X, Gold R, Thompson AJ et al. ECTRIMS/EAN Guideline on the pharmacological treatment of people with multiple sclerosis. Mult Scler 2018;24(2):96-120. https://doi.org/10.1177/1352458517751049
- Kister I, Bacon TE, Chamot E et al. Natural history of multiple sclerosis symptoms. Int J MS Care 2013;15(3):146-158. https://doi.org/10.7224/1537-2073.2012-053
- Bohannon RW, Smith MB. Interrater reliability of a modified Ashworth scale of muscle spasticity. Phys Ther 1987;67(2):206-207. https://doi.org/10.1093/ptj/67.2.206
- Haugh AB, Pandyan AD, Johnson GR. A systematic review of the Tardieu Scale for the measurement of spasticity. Disabil Rehabil 2006;28(15):899-907. https://doi.org/10.1080/09638280500404305
- Hobart JC, Riazi A, Thompson AJ et al. Getting the measure of spasticity in multiple sclerosis: the Multiple Sclerosis Spasticity Scale (MSSS-88). Brain 2006;129(Pt 1):224-234. https://doi.org/10.1093/brain/awh675
- Farrar JT, Troxel AB, Stott C, Duncombe P, Jensen MP. Validity, reliability, and clinical importance of change in a 0-10 numeric rating scale measure of spasticity: a post hoc analysis of a randomized, double-blind, placebo-controlled trial. Clin Ther 2008;30(5):974-985. https://doi.org/10.1016/j.clinthera.2008.05.011
- Otero-Romero S, Sastre-Garriga J, Comi G et al. Pharmacological management of spasticity in multiple sclerosis: Systematic review and consensus paper. Mult Scler 2016;22(11):1386-1396. https://doi.org/10.1177/1352458516643600
- Pozzilli C. Advances in the management of multiple sclerosis spasticity: experiences from recent studies and everyday clinical practice. Expert Rev Neurother 2013;13(12 Suppl):49-54. https://doi.org/10.1586/14737175.2013.865877
- Baker D, Pryce G, Jackson SJ, Bolton C, Giovannoni G. The biology that underpins the therapeutic potential of cannabis-based medicines for the control of spasticity in multiple sclerosis. Mult Scler Relat Disord 2012;1(2):64-75.
- Shakespeare DT, Boggild M, Young C. Anti-spasticity agents for multiple sclerosis. Cochrane Database Syst Rev 2003;(4):CD001332. https://doi.org/10.1002/14651858.CD001332
- Zajicek J, Fox P, Sanders H et al. Cannabinoids for treatment of spasticity and other symptoms related to multiple sclerosis (CAMS study): multicentre randomised placebo-controlled trial. Lancet 2003;362(9395):1517-1526. https://doi.org/10.1016/S0140-6736(03)14738-1
- Collin C, Davies P, Mutiboko IK, Ratcliffe S. Randomized controlled trial of cannabis-based medicine in spasticity caused by multiple sclerosis. Eur J Neurol 2007;14(3):290-296. https://doi.org/10.1111/j.1468-1331.2006.01639.x
- Wade DT, Makela PM, House H, Bateman C, Robson P. Long-term use of a cannabis-based medicine in the treatment of spasticity and other symptoms in multiple sclerosis. Mult Scler 2006;12(5):639-645. https://doi.org/10.1177/1352458505070618
- Pryce G, Baker D. Control of spasticity in a multiple sclerosis model is mediated by CB1, not CB2, cannabinoid receptors. Br J Pharmacol 2007;150(4):519-525. https://doi.org/10.1038/sj.bjp.0707003
- Corey-Bloom J, Wolfson T, Gamst A et al. Smoked cannabis for spasticity in multiple sclerosis: a randomized, placebo-controlled trial. CMAJ 2012;184(10):1143-1150. https://doi.org/10.1503/cmaj.110837
- Vaney C, Heinzel-Gutenbrunner M, Jobin P et al. Efficacy, safety and tolerability of an orally administered cannabis extract in the treatment of spasticity in patients with multiple sclerosis: a randomized, double-blind, placebo-controlled, crossover study. Mult Scler 2004;10(4):417-424. https://doi.org/10.1191/1352458504ms1048oa
- Novotna A, Mares J, Ratcliffe S et al. A randomized, double-blind, placebo-controlled, parallel-group, enriched-design study of nabiximols* (Sativex((R)) ), as add-on therapy, in subjects with refractory spasticity caused by multiple sclerosis. Eur J Neurol 2011;18(9):1122-1131. https://doi.org/10.1111/j.1468-1331.2010.03328.x
- Leocani L, Nuara A, Houdayer E et al. Sativex((R)) and clinical-neurophysiological measures of spasticity in progressive multiple sclerosis. J Neurol 2015;262(11):2520-2527. https://doi.org/10.1007/s00415-015-7878-1
- Trojano M, Vila C. Effectiveness and Tolerability of THC/CBD Oromucosal Spray for Multiple Sclerosis Spasticity in Italy: First Data from a Large Observational Study. Eur Neurol 2015;74(3-4):178-185. https://doi.org/10.1159/000441619
- Allan GM, Finley CR, Ton J et al. Systematic review of systematic reviews for medical cannabinoids: Pain, nausea and vomiting, spasticity, and harms. Can Fam Physician 2018;64(2):e78-e94.
- Schiavo G, Santucci A, Dasgupta BR et al. Botulinum neurotoxins serotypes A and E cleave SNAP-25 at distinct COOH-terminal peptide bonds. FEBS Lett 1993;335(1):99-103. https://doi.org/10.1016/0014-5793(93)80448-4
- Royal College of Physicians. Spasticity in adults: management using botulinum toxin. National Guidelines. 20-3-2018.
- Sammaraiee Y, Yardley M, Keenan L, Buchanan K, Stevenson V, Farrell R. Intrathecal baclofen for multiple sclerosis related spasticity: A twenty year experience. Mult Scler Relat Disord 2019;27:95-100. https://doi.org/10.1016/j.msard.2018.10.009
- Sadiq SA, Wang GC. Long-term intrathecal baclofen therapy in ambulatory patients with spasticity. J Neurol 2006;253(5):563-569. https://doi.org/10.1007/s00415-005-0060-4
- Lee BS, Jones J, Lang M et al. Early outcomes after intrathecal baclofen therapy in ambulatory patients with multiple sclerosis. J Neurosurg 2018;129(4):1056-1062. https://doi.org/10.3171/2017.5.JNS162925
- NathanDr Rachel Farrell, Neurorehabilitation, National Hospital of Neurology and Neurosurgery, Queen Square, London WC1N 3BG. PW, Sears TA, Smith MC. Effects of phenol solutions on the nerve roots of the cat: an electrophysiological and histological study. J Neurol Sci 1965;2(1):7-29. https://doi.org/10.1016/0022-510X(65)90060-2
- Gaid M. Phenol Nerve Block for Management of Lower Limb Spasticity. Advances in Neurological Science and Rehabilitation. 11-12-2012.
- Simeoni S, Keenan E, Lee H et al. Intrathecal phenol is a safe and effective treatment option for severe lower limb spasticity in advanced multiple sclerosis. Mult.Scler. 24, 596. 9-9-2018. https://doi.org/10.26226/morressier.5b719e475aff74008ae4cace