Lewis Katz School of Medicine at Temple University research shows Pison’s Neural Biosensor can potentially enable remote monitoring, early detection and intervention for neurological diseases
Pison have announced the results of recent clinical trial conducted by researchers at the Lewis Katz School of Medicine at Temple University’s MDA/ALS Center of Hope, in the US. The trials concluded that Pison’s Neural Biosensor hardware and electroneurography (ENG) technology was able to distinguish patients with amyotrophic lateral sclerosis (ALS) from a healthy population and detect changes in surface electromyography (sEMG) in ALS patients which reflects motor neuron changes and is correlated with functional changes. These results demonstrate that Pison’s technology has the potential to become a digital biomarker to detect neurological diseases, monitor progression, and inform treatment.
In addition, Pison’s ongoing efforts to embed their technology into wearable devices, such as smart watches, opens the door for continuous monitoring of patients and even pre-symptomatic populations.
The study, funded by The ALS Association and the National Science Foundation and led by Dr. Terry Heiman-Patterson, Professor of Neurology and Director of the MDA/ALS Center of Hope at the Lewis Katz School of Medicine at Temple University, used Pison’s technology to classify electromyography activity and fasciculations in patients in the early stages of ALS. The study found that Pison’s technology could distinguish between patients diagnosed with ALS and a healthy population.
New and better ways to diagnose and monitor people with ALS are urgently needed. We are proud to have supported the initial testing of this promising new technology. We look forward to seeing the results of future studies to confirm and validate these findings with larger groups of participants.
Dr. Kuldip Dave, Senior Vice President of Research at The ALS Association.
Researchers at the John P Hussman Institute for Human Genomics at the University of Miami Miller School of Medicine, US have found that variations in chromatin accessibility, and thus gene expression, may explain why people of European descent with APOE4 gene variants have a greater risk of developing Alzheimer’s disease than people of African descent with similar genetics. The study was published on April 10 2023 in the journal Alzheimer’s & Dementia.
“We previously showed that people with European ancestry have higher APOE4 expression than their African counterparts, but we didn’t understand why,” said Jeffery Vance M.D., Ph.D.,
Professor and Director, Center for Genomic Education & Outreach, John P. Hussman Institute for Human Genomics and senior author on the study. “Now, we know that differences in how the DNA is packaged – chromatin accessibility – contribute to these distinctions.”
Cells pack a lot of DNA into a small area – around six feet of genetic material per cell if it were unwrapped and extended. Tight packaging is a necessity, but it also impacts gene expression. Chromatin, the mixture of DNA and proteins that make up chromosomes, plays a major role in unpacking specific DNA regions to support expression. As a result, chromatin accessibility is profoundly important for both good health and disease.
In the study, the team investigated chromatin in astrocytes from 12 brains (six European and six African Americans) impacted by Alzheimer’s disease. All the African Americans had inherited APOE4 from an African ancestor. Astrocytes are neural housekeeping cells that support neuronal function and many other areas. They are also deeply implicated in Alzheimer’s disease progression.
drug and diagnostics companies may want to reconsider how they conduct clinical trials, as patients may present entirely different risk profiles based on their ancestry.
The team found increased accessibility in European astrocytes, boosting the expression of APOE4, as well as genes associated with synapses (the space between neurons), cholesterol and astrocyte reactivity.
While these results provide insights into an important question about APOE4 function in European and African genomes, they also generate complex issues surrounding descent and health risks.
“When we look at African American ancestry, many who consider themselves Black have significant numbers of genes from European descendants,” said Katrina Celis, M.D., an Associate Scientist from the Hussman Institute and first author on the study. “Both African Americans and Hispanic/Latino Americans are admixed populations, with a patchwork of ancestries across each chromosome.”
As a result, people from these groups could inherit their APOE4 gene from African, European, Hispanic/Latino or Amerindian ancestors. Their Alzheimer’s disease risk from APOE4 depends on the ancestry surrounding it, which will affect their APOE4 expression.
These findings could inform clinical care, diagnostics and therapeutics. Clinicians may need to understand a patient’s ancestral profile before assessing the risks associated with their APOE4 status.
In addition, drug and diagnostics companies may want to reconsider how they conduct clinical trials, as patients may present entirely different risk profiles based on their ancestry. These new insights could also lead to better Alzheimer’s drugs.
“Because we now know there’s a difference in accessibility and expression, APOE4 itself could become a therapeutic target,” said Dr. Vance. “Current options target amyloid plaques with limited success. New avenues of therapeutic intervention are needed, and APOE4 is a key target as we move ahead.”
Scientists at Sylvester Comprehensive Cancer Center at the University of Miami Miller School of Medicine, US collaborating with international researchers, have developed a sophisticated AI algorithm that performs advanced computational analysis to identify potential therapeutic targets for glioblastoma multiforme (GBM) and other cancers.
“Our work represents translational science that offers immediate opportunities to change the way glioblastoma patients are routinely managed in the clinic,” explained Antonio Iavarone, M.D., deputy director of Sylvester Comprehensive Cancer Center and senior author of the study. “Our algorithm offers applications to precision cancer medicine, giving oncologists a new tool to battle this deadly disease and other cancers as well.”
The AI algorithm, known as SPHINKS – Substrate PHosphosite-based Inference for Network of KinaseS – deployed deep-machine learning to help the researchers identify and experimentally validate two protein kinases (PKCδ and DNAPKcs) as the culprits associated with tumor progression in two GBM subtypes and as potential therapeutic targets for other cancers.
Protein kinases are the key targets currently used in precision cancer medicine to tailor treatment to a patient’s specific cancer properties. The most active kinases, which the researchers labeled “master kinases” in their paper, are those for which clinicians direct targeted drugs as a hallmark of current cancer treatment.
In addition to identifying the master kinases, Dr. Iavarone and colleagues used tumor organoids grown in the laboratory from patient samples – what they called “patient-derived tumour avatars” – to show that targeted drugs that interfere with the activity of master kinases can thwart tumor growth.
Previously, Dr. Iavarone and team had reported a new glioblastoma classification by capturing key tumor cell traits and grouping GBM patients based on their likelihood of survival and their tumor’s vulnerability to drugs. In the new study, these classifications were independently confirmed through several omics platforms: genomics (genes), proteomics (proteins) lipidomics (fat molecules), acetylomics (epigenetics), metabolomics (metabolites) and others.
SPHINKS leverages machine learning to refine these omics datasets and create an interactome –a complete set of biological interactions – to pinpoint the kinases that generate aberrant growth and treatment resistance in each glioblastoma subtype. These findings show multi-omics data can generate new algorithms that predict which targeted therapies can provide the best therapeutic options based on each patient’s glioblastoma subtype.
“We can now stratify glioblastoma patients based on biological features that are common between different omics,” Dr. Iavarone said. “Reading the genome alone has not been enough. We have needed more comprehensive data to identify tumour vulnerabilities.”
Despite breakthroughs for many other cancers, glioblastoma patients face dismal prognoses – the five-year survival rate is below 10%. Although numerous drugs are being developed as potential therapy, clinicians have needed a way to identify the molecular mechanisms that drive each patient’s disease and are applicable to precision cancer medicine.
The SPHINKS algorithm and related methods can be readily incorporated into molecular pathology labs, according to the researchers. Their paper includes a clinical classifier that can help assign the appropriate glioblastoma subtype to each patient. The team has also established an online portal to access the algorithm. The authors believe this approach can produce insightful information that could benefit as many as 75% of glioblastoma patients.
This classifier can be used in basically any lab. By importing the omics information into the web portal, pathologists receive classification information for one tumor, ten tumors, however many they import. These classifications can be applied immediately to patient care.
Anna Lasorella, M.D., professor of biochemistry and molecular biology at Sylvester CCC and co-senior author on the study.
While SPHINKS was first tested on glioblastoma, the algorithm is equally applicable to several other cancers. The team found the same cancer-driving kinases in breast, lung and pediatric brain tumors. Drs. Iavarone and Lasorella and colleagues believe this finding could be the impetus for a new type of clinical trial.
“We are exploring the concept of basket trials,” Dr. Iavarone explained, “which would include patients with the same biological subtype but not necessarily the same cancer types. If patients with glioblastoma or breast or lung cancer have similar molecular features, they could be included in the same trial,” he continued. “Rather than doing multiple trials for a single agent, we could conduct one combined trial and potentially bring more effective drugs to more patients faster.”
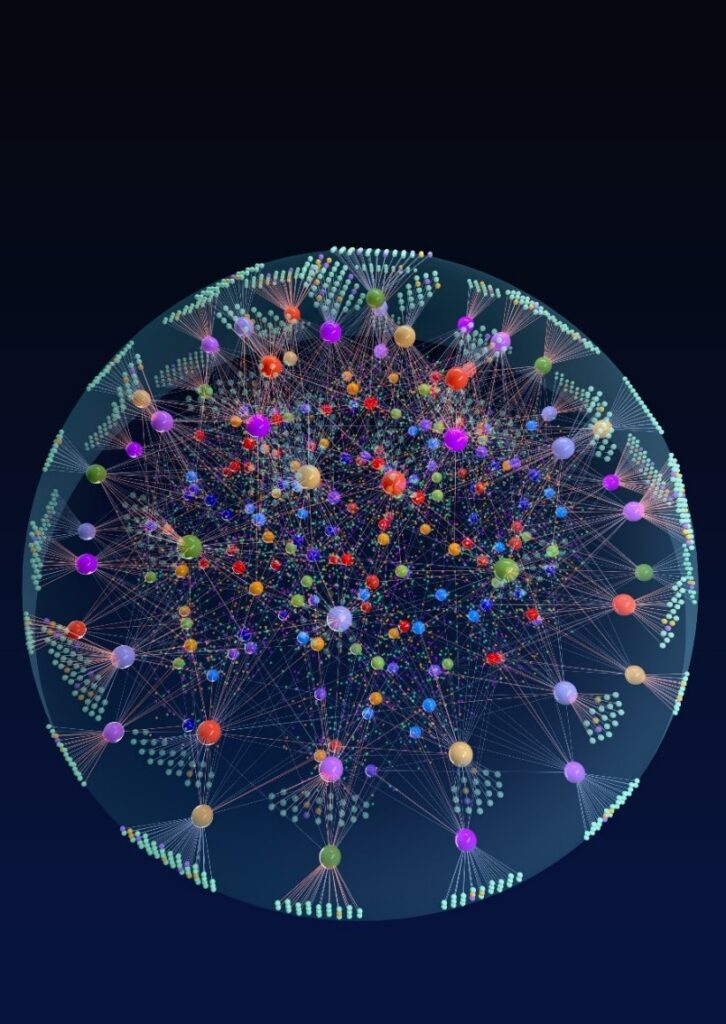
The image shows the SPHINKS network for the precision targeting of master kinases in glioblastoma. Credit: Antonio Iavarone, M.D.
This work was supported by National Institutes of Health grant nos. U54CA193313, R01CA239721 and R01CA268592 (to A.L.); U54CA193313, R01CA190891, R01CA268592, R01CA239698 and R35CA253183; NCI P30 Supplement GBM CARE-HOPE; the Chemotherapy Foundation (to A.I.); and the Italian Association for Cancer Research Project IDs 21846 (IG) and 21073 (5 per mille) (to M.C.). S.M. is recipient of a fellowship from the Italian Association for Cancer Research.
Drs. Lasorella and Iavarone are inventors of a biomarker technology that has been licensed to QIAGEN. Dr. Iavarone received sponsored research funding from AstraZeneca and Taiho Pharmaceutical and has served as a paid consultant/advisor to AIMEDBIO. Dr. Lasorella received sponsored research funding from Celgene. Both are inventors of a patent application based on this work. All other authors declare no competing interests.
MycarinG study publication reports the clinically meaningful and statistically significant effects of rozanolixizumab across key endpoints in adult patients with acetylcholine receptor autoantibody positive (AChR-Ab+) or muscle-specific tyrosine kinase (MuSK-Ab+) autoantibody positive gMG, in the largest study in patients with gMG to date.
RAISE publication describes clinically meaningful and statistically significant improvements in MG-specific efficacy outcomes, as well as a favorable safety profile, for zilucoplan, the first C5 complement inhibitor to be self-administered at home by adult patients with AChR-Ab+ gMG.
Rozanolixizumab and zilucoplan are investigational therapies currently under regulatory review in the U.S., Europe and Japan.
13 April 2023: UCB, a global biopharmaceutical company, announced that The Lancet Neurology has published data from the Phase 3 MycarinG study evaluating the efficacy and safety of rozanolixizumab in adult patients with acetylcholine receptor autoantibody-positive (AChR-Ab+) or muscle-specific tyrosine kinase autoantibody-positive (MuSK-Ab+) generalised myasthenia gravis (gMG) and the Phase 3 RAISE study evaluating the efficacy and safety of zilucoplan in adult patients with mild to severe AChR-Ab+ gMG.1,2
UCB is investigating both therapies as part of a broad offering to treat adult patients living with gMG throughout their treatment journey; each has an individual mechanism of action targeting the underlying disease pathology that causes gMG.
The safety and efficacy of rozanolixizumab and zilucoplan have not been established and neither treatment is approved for use in any indication by any regulatory authority worldwide.
There is an ongoing need for well-tolerated, targeted treatment options to improve the quality of life of people living with gMG. Many of the current treatment options only offer symptomatic relief which results in a treatment burden in addition to the already substantial disease burden. These papers published in The Lancet Neurology further reinforce the potential of rozanolixizumab and zilucoplan – with their different MOAs – to provide targeted treatment options to patients to help them manage fluctuating and unpredictable symptoms both at home and in a healthcare setting.
Iris Loew-Friedrich, Executive Vice-President and Chief Medical Officer at UCB.
In the MycarinG study1 (n=200) – the largest gMG population Phase 3 study published to date – in adult patients with AChR-Ab+ or MuSK-Ab+ gMG, rozanolixizumab demonstrated statistically significant and clinically meaningful improvements in MG-specific outcomes in patients with MuSK-Ab+ or AChR-Ab+ gMG, that were consistent with prior published results. Reductions in MG-ADL score from baseline to day 43 were greater in the rozanolixizumab 7 mg/kg group (least-squares mean change –3·37 [SE 0·49]) and in the rozanolixizumab 10 mg/kg group (–3·40 [0·49]) than with placebo (–0·78 [0·49]; for 7 mg/kg, least-squares mean difference −2·59 [95% CI −4·09 to −1·25], p<0·0001; for 10 mg/kg, −2·62 [−3·99 to −1·16], p<0·0001). In the MuSK-Ab+ specific subgroup, improvement in MG-ADL was –7.28 (7mg/kg; n=5), –4.16 (10mg/kg; n=8), and 2.28 (placebo; n=8). In the AChR-Ab+ specific subgroup, improvement in MG-ADL was –3.03 (7mg/kg; n=60), –3.36, (10mg/kg; n=60), and –1.10 (placebo; n=59).
Both rozanolixizumab doses were generally well tolerated with similar occurrences of TEAEs between both doses. The most frequently reported TEAEs were headache, diarrhea, and pyrexia. A higher incidence of headache was reported in the rozanolixizumab groups versus placebo, with most cases mild to moderate and severe cases generally managed with non-opioid analgesics. Treatment discontinuation rates due to TEAEs were low.
Importantly, the MycarinG study included Patient-Reported Outcomes (PROs) measures as secondary endpoints. The novel Myasthenia Gravis Symptoms PRO (MGS-PRO) – a measure used to assess symptom severity and impact of MG on patient lives, including physical fatigue which is not covered in other MG clinical outcome assessments – demonstrated statistically significant results vs placebo.
“The findings from the MycarinG study support the mechanism of action of neonatal Fc receptor inhibition and the potential for rozanolixizumab in adult patients with acetylcholine receptor autoantibody positive (AChR-Ab+) or muscle-specific tyrosine kinase (MuSK-Ab+) autoantibody positive generalised myasthenia gravis,” explained Professor Vera Bril, Professor of Medicine (Neurology), University of Toronto, Director of the Neuromuscular Section, Division of Neurology, University of Toronto and University Health Network, Toronto, and lead investigator of the MycarinG study. “Rozanolixizumab showed clinically meaningful improvements in patient-reported and investigator-assessed outcomes for both 7 mg/kg and 10 mg/kg doses. Both doses were generally well tolerated. If approved in the future, rozanolixizumab represents a potential additional treatment option for adult patients with generalised myasthenia gravis.”
In the RAISE study2 (n=174), in adult patients with mild to severe AChR-Ab+ gMG, zilucoplan demonstrated rapid efficacy, with consistent, sustained, clinically meaningful and statistically significant improvements versus placebo from baseline to week 12 in both patient and clinician-reported endpoints, including MG-ADL, which was the primary efficacy endpoint, and QMG, MGC and MGQoL15, which were secondary efficacy endpoints (the threshold for clinically meaningful MG-QoL15r has not yet been established).2 At Week 12, more patients receiving zilucoplan, achieved a ≥3-point reduction in MG-ADL score without rescue therapy, compared with those receiving placebo (73% and 46%, respectively; odds ratio [95% CI] = 3·18 [1·66, 6·10]; p=0·0005;). Additionally, more patients receiving zilucoplan, compared with those receiving placebo, (58% and 33%, respectively) achieved a ≥5-point reduction in QMG score without rescue therapy at Week 12 (odds ratio [95% CI] = 2·87 [1·52, 5·40]; p=0·0012;).
Zilucoplan was generally well tolerated with a favorable safety profile. The most frequently reported TEAEs in the zilucoplan group were injection site bruising, headache, diarrhea, and (worsening of) MG.2 Incidences of serious TEAEs and serious infections were similar in both groups. All patients who completed the 12-week treatment period (n=166) chose to enroll in RAISE-XT, the ongoing open label extension study.2 If approved, zilucoplan would be the first C5 complement inhibitor in gMG that patients can self-administer at home.
“In the RAISE study, zilucoplan showed rapid and clinically meaningful improvements in myasthenia gravis-specific efficacy outcomes, had a favorable safety profile, and was generally well tolerated, with no major safety findings,” said James F. Howard, MD, Distinguished Professor of Neuromuscular Disease, Professor of Neurology, Medicine and Allied Health, The University of North Carolina at Chapel Hill School of Medicine and lead investigator in the RAISE trial. “These results suggest that, if approved in the future, zilucoplan could present a potential new treatment option for a broad population of adult patients with AChR-Ab+ generalised myasthenia gravis.”
Earlier this year, the US Food and Drug Administration (FDA) accepted UCB’s filing to review a Biologic License Application (BLA) for rozanolixizumab for the treatment of gMG in adult patients. The BLA was designated for Priority Review, with a response from the agency anticipated in Q2 2023. This BLA followed the European Medicines Agency’s (EMA) validation of the Marketing Authorization Application (MAA) for rozanolixizumab, and the FDA’s acceptance of a New Drug Application (NDA) and the EMA’s validation of the MAA for zilucoplan in the same indication. Regulatory applications for rozanolixizumab and zilucoplan for the treatment of gMG have also been filed in Japan. Responses from regulatory agencies to these submissions are expected in H2 2023.
“Our ultimate goal is to provide targeted treatment options that can help reduce the ongoing daily burden of gMG, giving patients additional flexible treatment options that work alongside their daily life,” said Charl van Zyl, Executive Vice President Neurology Solutions & Head of EU/International Markets, UCB. “With measures such as MGS-PRO in the MycarinG study, we have been able to see the positive impact rozanolixizumab has had on patient experience, while results from the RAISE study demonstrated the potential of zilucoplan as an effective and generally well-tolerated treatment that can be self-administered at home, giving people greater independence. These results bring us one step forward towards offering tailored options to meet individual patient needs.”
gMG is a rare, chronic, heterogeneous (phenotypic and pathogenic), and unpredictable auto-immune disease characterised by dysfunction and damage at the neuromuscular junction.3 Several factors are understood to be drivers of gMG disease pathology, including complement, immune cells and pathogenic IgG autoantibodies.4
People living with gMG can experience a variety of symptoms, including drooping eyelids, double vision, and difficulty in swallowing, chewing and talking, as well as severe muscle weakness that can result in life-threatening weakness of the muscles of respiration.5,6 MG is a rare disease with a global prevalence of 100–350 cases per every 1 million people.7
Hansen JS, et al. Mortality in myasthenia gravis: A nationwide population-based follow-up study in Denmark. Muscle Nerve. 2016; 53: 73-77.
Punga, Anna Rostedt et al. “Epidemiology, diagnostics, and biomarkers of autoimmune neuromuscular junction disorders.” The Lancet. Neurology vol. 21,2 (2022): 176-188. doi:10.1016/S1474-4422(21)00297-0
ClinicalTrials.gov ‘A Study to Test Efficacy and Safety of Rozanolixizumab in Adult Patients With Generalized Myasthenia Gravis’: https://clinicaltrials.gov/ct2/show/NCT03971422. Accessed February 2023.
Kiessling P, et al. The FcRn inhibitor rozanolixizumab reduces human serum IgG concentration: A randomized Phase 1 study. Sci Transl Med. 2017;9(414:eaan1208).
Smith B, et al. Generation and characterization of a high affinity anti-human FcRn antibody, rozanolixizumab, and the effects of different molecular formats on the reduction of plasma IgG concentration. MAbs. 2018;10:1111-1113.
ClinicalTrials.gov ‘Safety, Tolerability, and Efficacy of Zilucoplan in Subjects With Generalized Myasthenia Gravis (RAISE)’: https://clinicaltrials.gov/ct2/show/NCT04115293. Accessed March 2023.
Fully enrolled phase III Evobrutinib studies continue
The US Food and Drug Administration (FDA) has placed a partial clinical hold on the initiation of new patients on evobrutinib and patients with less than 70 days exposure to study medication in the US.
12 April 2023: Merck today announced the US Food and Drug Administration (FDA) has placed a partial clinical hold on the initiation of new patients on evobrutinib and patients with less than 70 days exposure to study medication in the US. The ongoing, fully-enrolled Phase III EVOLUTION clinical trial programme of evobrutinib in relapsing multiple sclerosis (RMS) will continue as planned with all participants remaining on treatment as all are beyond 70 days exposure to study medication.
The Phase III clinical trial programme of evobrutinib is on schedule to read out in the fourth quarter of 2023.
The FDA action was based on their assessment of two recently reported cases of laboratory values suggestive of drug-induced liver injury that have been identified during the Phase III studies. Importantly, both patients were asymptomatic, did not require any medical intervention or hospitalisation for this condition and their liver enzymes fully normalised after discontinuation of the study medication.
The Phase III EVOLUTION clinical trial programme of evobrutinib has been closely monitored by an Independent Data Monitoring Committee, including hepatologists, since initiation. In close collaboration with external experts as well as the Independent Data Monitoring Committee for the trials, Merck is assessing the potential contributory role of predisposing factors to the liver injury.
Merck is working closely with the FDA to establish the best path forward for the benefit of patients in current and future trials with evobrutinib.
About Evobrutinib
Evobrutinib is an oral, CNS-penetrating, highly selective inhibitor of Bruton’s tyrosine kinase (BTK) in clinical development as a potential treatment for relapsing multiple sclerosis (RMS). It is the first BTK inhibitor (BTKi) to demonstrate clinical efficacy in the largest Phase II study with follow-up beyond three years as well as demonstrate an impact on early biomarkers of ongoing central inflammation that correlate with disease progression, including slowly expanding lesions (SEL) volume and levels of blood neurofilament light chain protein (NfL). Evobrutinib is designed to modulate B cell responses such as proliferation and antibody and cytokine release, as well as modulate macrophage/microglia activation. During Phase II, the BTKi dose finding study demonstrated that BID dosing achieved maximal efficacy with >95% BTK occupancy maintained in 98% of patients before the next dose. Evobrutinib is currently under clinical investigation and is not approved for any use anywhere in the world.
Phase two trial saw significant reduction in pressure in the brain and monthly headaches
Study first to show rapid reduction in brain pressure in first 24hrs of treatment
March 13, 2023: Patients with ‘blinding’ headaches known as Idiopathic Intercranial Hypertension (IIH) could be treated with an injectable peptide used for type 2 diabetes, a new trial has found.
The study, published in the journal Brain, reports on a phase two trial of a drug called exenatide, a GLP-1 receptor agonist, as a potential treatment for IIH.
The IIH Pressure Trial led by a team of neurologists from the University of Birmingham and University Hospitals Birmingham found that for the seven patients who received regular injections of the drug, currently approved for use in Type 2 Diabetes, led to a drop in pressure in the brain during both short (2.5hrs and 24hrs) and long term (12 weeks) measurements.
The trial also saw significant reductions in the numbers of headaches across the 12 weeks that participants took part, with an average of 7.7 fewer days per month of headaches compared to the baseline, compared to only 1.5 fewer days in the placebo arm.
Alex Sinclair is Professor of Neurology in the Institute of Metabolism and Systems Research at the University of Birmingham, an Honorary Consultant Neurologist at University Hospitals Birmingham NHS Foundation Trust, and Principal Investigator of the study.
This is a major trial for the rare and debilitating condition IIH that can lead to people, usually women, going blind and suffering disabling daily headaches. There are no current licenced drugs to treat IIH and hence this result is a major step forward for IIH patients.
Professor Alex Sinclair
“We are delighted to see that the phase two trial resulted in our treatment group having lower brain pressure both immediately and after 12 weeks and nearly 8 fewer headache days across the 12-week period, and that all the women were able to continue the treatment throughout with few adverse effects. We now hope to see a much larger trial of exenatide to literally ease the pressure for the many people around the world suffering with IIH.”
Shot in the arm for IIH treatment
Idiopathic Intracranial Hypertension (IIH) is a debilitating condition that raises pressure in the brain and can lead to chronic headaches and even permanent sight loss. The illness, which often leaves patients with a reduced quality of life, predominately affects women aged 25 to 36 and weight gain is a major risk factor of developing IIH and relapses of the disease.
Once regarded as rare, incidence of IIH is now rising dramatically in line with the global rise in obesity and there has been a 350 per cent rise in incidence in last 10 years. Currently there are no licenced drugs options and existing medications used off label are complicated by troublesome side effects.
A key finding was the rapid action of the drug, with results indicating that brain pressure was significantly reduced within two and half hours of taking the medication. This rapid onset of action is vital in a condition which can cause rapid blindness if left untreated.
Dr James Mitchell, Lecturer in Neurology at the University of Birmingham and first author of the paper said:
“The results of this clinical trial are a shot in the arm for finding clinical treatments for IIH. While we need to do further trials before such a treatment could be available for patients in the future, we are encouraged by the significant results from this trial that made a real difference for those in the treatment arm and this treatment may prove relevant for other conditions resulting in raised brain pressure.”
In this study the drug was given as a twice daily injection into the subcutaneous tissue. To reduce the need for frequent injection in the future a once weekly subcutaneous injection called Presendin will be trialled though University of Birmingham Start-up company, Invex Therapeutics.
Shelly Williamson, the Chair of patient charity IIH UK said:
“This is such exciting progress. New drug options is vitally important for IIH and this trial brings hope to the millions of patients living with the condition. We very much look forward to the next steps and seeing the drug tested in two large Phase 3 clinical trials.”
The IIH Advance is a Phase 3 clinical trial in Adolescents run in the UK, sponsored by the University of Birmingham and IIH Evolve is running in adults internationally sponsored by Invex Therapeutics. Ultimately the aim is to gain enough evidence to allow the drug to be licensed for use in IIH patients in the future.
Queen Mary and icometrix have together been awarded the prestigious AI Award in Health and Care by the National Institute for Health and Care Research (NIHR)
7th March 2023
The collaborative programme will investigate the impact of AI on the assessment of MRI and decision making for people with multiple sclerosis (MS). It is hoped that this research will lead to better care for people with MS.
AssistMS will focus on the reporting of MRI by neuroradiologists in routine clinical practice. People with MS receiving disease-modifying treatments (DMT) undergo annual MRI of the central nervous system to monitor disease activity. This allows clinicians to detect whether the DMT is working or not. MRI is much more sensitive than clinical indices, and detecting disease activity early enables changing DMT such that MRI-detectable disease activity does not lead to clinical deterioration. However, detecting the often subtle changes on MRI is time-consuming, tiring and, consequently prone to human error.
The software tested in AssistMS, icobrain ms, detects and highlights subtle changes on brain MRI and provides summary reports. The hope is that the technology will enable clinicians to make better informed DMT. Clinicians will be able to detect signs of disease activity faster and more effectively, enabling them to make quicker decisions about a possible DMT switch.
As part of AssistMS, neuro-radiologists and radiologists will perform their assessment with and without the support of icobrain ms. The project will investigate the accuracy and the consistency of the AI tool in detecting disease activity and other clinically important features in MRI brain images from about 1300 people with MS cared for in east London and Nottingham.
The project is expected to start in the coming months and will run for three years.
I am thrilled about this generous award funded by NIHR through the NHS AI Lab’s AI in Health and Care Award. If successful, AssistMS will have a significant impact on people with MS’ quality of life as well as equity and efficiency of MS care across the UK
Klaus Schmierer, Professor of Neurology at Queen Mary and joint lead of AssistMS
On March 30th 2023 Cognito Therapeutics announced neuroimaging results evaluating the effects of the company’s non-invasive neuromodulation medical device, which delivers proprietary gamma frequency light and sound stimulation in participants with Alzheimer’s disease (AD). The results were presented at the AD/PD™ 2023 International Conference on Alzheimer’s and Parkinson’s Diseases and related neurological disorders, on March 28–April 1, 2023 in Gothenburg, Sweden.
Neuroimaging data was prospectively collected in the OVERTURE clinical trial (NCT03556280) along with safety, tolerability, and efficacy of Cognito Therapeutics’ medical device in participants with Alzheimer’s disease. 76 participants were randomised 2:1 to receive daily, one-hour, EEG-assessed, proprietary non-invasive neuromodulation (active arm, n=46) or sham (placebo arm, n=28) stimulation over a 6-month period. AD brain pathological changes were evaluated by neuroimaging methods, including volumetric MRI and [18]florbetapir PET.
Results
A significant reduction in whole brain volume loss was observed, which correlated with reduced lateral ventricle expansion, in subjects in the active compared to the sham group. The active group also showed a significantly reduced loss in white matter volume, occipital lobe volume and cortical thickness. Volumetric changes showed correlations between brain regions and clinical outcomes, prominently between occipital lobe and activity of daily living (ADCS-ADL). Although neither the active nor the sham arm participants showed a significant difference in amyloid plaque load, Cognito’s proprietary neuromodulation was effective in both amyloid positive and negative subjects, including maintaining cognitive and functional efficacy outcomes.
The results presented at AD/PD 2023 from our Phase 2 OVERTURE clinical trial show that daily at-home use of our medical device decreases brain atrophy in Alzheimer’s patients. Our innovative approach, utilising non-invasive neuromodulation and neuroimaging methods, has yielded impressive results, including a significant reduction in whole brain MRI volume loss and potentially improved clinical outcomes. We are particularly encouraged by the correlations between reduced brain volume loss and clinical outcomes, as well as the impact of our therapy on both amyloid positive and negative patients. These findings indicate a potential breakthrough in Alzheimer’s research and provide hope for the millions of individuals and families affected by this disease. We remain committed to advancing our research and development efforts in bringing our innovative neurotechnology device to patients.
Brent Vaughan, CEO, Cognito Therapeutics.
Cognito Therapeutics is a clinical-stage neurotechnology company developing disease-modifying therapeutic approaches to treat neurodegenerative disorders. Its non-invasive neuromodulation platform was developed by MIT Professors and scientific founders Li-Huei Tsai and Ed Boyden. The Company’s lead therapy is currently in a pivotal study in Alzheimer’s Disease and was awarded FDA Breakthrough Device Designation. Cognito is based in Cambridge, MA. For more information, visit www.cognitotx.com.
In a paper published online on March 14th 2023 in the Journal of Parkinson’s Disease, researchers suggest that a common chemical, TCE, may be a key reason for the dramatic increase in Parkinson’s disease (PD).
Lead investigator Ray Dorsey, MD, professor of neurology, University of Rochester, US has called PD “the world’s fastest-growing brain disease,” and said it “may be largely preventable”.[1] TCE has been used in industry, commerce, military, and medicine, including producing refrigerants, cleaning electronics, and degreasing engine parts.
It has also been used in dry cleaning, although a similar chemical (perchloroethylene [PCE]) is more commonly used. However, the authors note that in anaerobic conditions, perchloroethylene often transforms into TCE “and their toxicity may be similar.” TCE is also found in consumer products such as paint removers and aerosol cleaning products and it was used to decaffeinate coffee until the 1970s.
TCE affects those who work with it, but it also pollutes outdoor air, taints groundwater, and contaminates indoor air. It is present in a substantial amount of US groundwater and it “evaporates from underlying soil and groundwater and enters homes, workplaces, or schools, often undetected,” the researchers note.
Sign up to receive our email newsletter with links to the latest content. ACNR is free, thanks to the support of advertisers. The editorial content is peer reviewed and remains completely independent unless clearly specified.