Ocrelizumab (Ocrevus®) has been accepted for use within NHS Scotland, for the treatment of adult patients with early primary progressive multiple sclerosis (PPMS) in terms of disease duration and level of disability, and with imaging features characteristic of inflammatory activity.
In a randomised, double-blind, phase III study, the risk of disability progression was significantly reduced in patients who received ocrelizumab compared with placebo.
Following many years of dedication and hard work by our scientists and the wider scientific community, today’s news is a landmark in the treatment of multiple sclerosis. People in Scotland with early, primary progressive multiple sclerosis (PPMS) will now be able to benefit from the first ever licensed treatment on the Scottish NHS. This underlines our commitment to support people in Scotland, across all of the diseases we cover, to live longer and healthier lives. We are proud to have again worked together with key Scottish stakeholders to make this happen.
On 13th January, 2020 the Scottish Medicines Consortium (SMC) announced that Fremanezumab (Ajovy) has been accepted for restricted use within NHS Scotland, for the treatment of adults with chronic and episodic migraine who have had prior failure on three or more migraine preventive treatments.
Ajovy, from Teva Pharmaceuticals, is the first dedicated migraine preventive medication that will be available to treat both chronic and episodic migraine.
It is a new class of drug which works by inhibiting a small protein found in nerve cells called calcitonin gene-related peptide (CGRP), which is believed to be involved in causing the pain in migraine attacks.
Scotland is the only nation in the UK where CGRP inhibitors have been approved to treat migraine on the NHS.
BERLIN & WEXFORD, PENNSYLVANIA, January 6, 2020 – ATAI Life Sciences AG (“ATAI” or the “Company”) today announced that it has partnered with Neuronasal Inc., to develop a short-term treatment for mild Traumatic Brain Injury (mTBI) or concussion.
Neuronasal’s potentially ground-breaking, proprietary treatment includes the intranasal delivery of low doses of N-acetylcysteine (NAC) to patients with acute mTBI. NAC is a well-established compound that has been used safely for decades, mostly as a mucolytic and to treat acute paracetamol intoxication. NAC is a precursor of cysteine, stimulating the synthesis of glutathione which in turn is the most abundant endogenous antioxidant, known to prevent oxidative damage to cellular components. In addition, NAC itself has direct antioxidant, anti-inflammatory, and free radical scavenging effects. Finally, NAC acts as an inhibitory glutamatergic modulator. All of these mechanisms are important in the context of mTBI.
Concussions and other forms of TBI represent a significant unmet medical need. With no currently approved treatments, patients not only suffer the typical acute symptomatology including headache, nausea, fatigue, depression, anxiety and irritability. In fact, approximately half of the 2.5 million people who are concussed every year in the United States alone develop long-term cognitive impairment. Also, the ongoing NINDS-funded track-TBI initiative has recently revealed that concussion is associated with substantial increases in the rates of major depressive disorder, post-traumatic stress disorder, and other psychiatric and non-psychiatric conditions.
“It’s clear that concussions and other mTBIs are more than just uncomfortable,” said Dr. Matthias Luz, Chief Medical Officer of ATAI Life Sciences. “In the hours and days after trauma, these injuries trigger a pathophysiological cascade that can result in significant, life-limiting conditions if not adequately addressed.”
Typically, concussions are the result of physical trauma that disrupts brain tissue and blood supply, followed by focal vascular leakage, inflammation, the formation of reactive oxygen species (ROS) and the release of excessive amounts of glutamate. This, in turn, exhausts the pool of intracellular glutathione in brain and induces glutamate-mediated neuro-excitotoxic damage. In more severe cases, neuronal atrophy and necrosis can occur as well.
NAC has the potential to disrupt the deleterious chain of events following mTBI. In soldiers exposed to explosive blast injury, NAC treatment, as compared to placebo, increased the probability of symptom resolution at 7 days from 41.9 to 86.2% when administered within 24 hours post-blast.
A particular problem with the use of NAC is the blood-brain barrier which effectively shields the brain from many drugs including NAC. When administered orally, several grams of NAC are required to reach the requisite drug concentrations in brain, doses which often cause significant side effects like nausea and diarrhea. Intravenous drug administration allows for slightly lower doses but requires several days of inpatient care and often leads to dizziness and headache.
By contrast, Neuronasal’s intranasal approach enables direct nose-to-brain delivery, allowing for significantly lower doses and outpatient treatment. Given its apparent efficacy in disrupting the underlying neurochemical cascade, intranasal NAC has the potential to induce a fundamental shift in the natural course of the condition for hundreds of thousands of people.
Neuronasal has the potential to transform the way we treat those most at risk of mTBI, with applications in sports, the military, and daily life. Unsurprisingly, we’ve seen incredible interest from everyone from the Department of Defense to the National Collegiate Athletic Association.
Thomas Bradshaw, CEO of Neuronasal
A pilot study exploring the effects of intranasal NAC administration on regional brain glutathione concentrations in healthy volunteers is expected to begin in February.
About ATAI Life Sciences
ATAI Life Sciences AG is a global biotech platform and company builder founded by Christian Angermayer. Based in Berlin, London and New York, its vision is to cure mental health disorders, enabling people to live healthier and happier lives. www.atai.life
Authorised for patients who have not responded to at least two different treatments with antidepressants in the current moderate to severe depressive episode and in combination with a Selective Serotonin Reuptake Inhibitor (SSRI) or Serotonin and Norepinephrine Reuptake Inhibitor (SNRI)
Esketamine nasal spray offers the first new mechanism of action in 30 years to treat major depressive disorder (MDD)
European Commission (EC) authorisation is based on data from a robust clinical trial programme in adult patients with treatment-resistant major depressive disorder (TRD), including five phase III trials
“This new treatment represents an exciting new therapeutic option for a common, debilitating and difficult to treat condition,” says Professor Allan Young, Chair of Mood Disorders and Director of the Centre for Affective Disorders, King’s College London.* “I believe both clinicians and patients will welcome this treatment option for this often-devastating illness.”
MDD affects approximately 40 million people across Europe and 1.8 million adults in England alone.[ii],[iii],—[iv] It is a major health condition that is recognised as the most common mental health condition in Europe that causes significant ill-health, disability and suffering for patients and their families.[v],[vi] People with MDD can suffer with episodes for many months or even years before being diagnosed and the effects go beyond the psychiatric and physical symptoms.[vii] It may also affect employment and education, relationships, health and overall quality of life.[viii] One-third of people in Europe living with MDD are considered to have TRD, that can cause significantly lower health-related quality of life, reduced productivity at work and increased absenteeism.[ix],[x]
“The marketing authorisation of esketamine nasal spray is a testament to Janssen’s dedication to improving outcomes for people struggling to overcome the devastating effects of treatment-resistant major depressive disorder,” said Bernardo Soares, Medical Director UK, Janssen-Cilag Ltd. “We are proud to be introducing this innovative treatment option, which we hope will help to address a significant unmet need.”
The European marketing authorisation was based on data from a robust clinical trial programme in patients with TRD, including over 1,600 patients treated with esketamine nasal spray. The five phase III trials included three short-term studies, one randomised withdrawal and maintenance of effect study, and one long-term safety study.[xi],[xii],[xiii],[xiv],—[xv]
The short-term (one-month) flexible dosing study in adults under 65 years of age demonstrated statistically significant reductions in depressive symptoms at 28 days for esketamine nasal spray and oral antidepressant compared to oral antidepressant and placebo nasal spray. Approximately 70 percent of esketamine nasal spray-treated patients responded to treatment, with a ≥50 percent symptom reduction. Furthermore, approximately half of all esketamine nasal spray-treated patients achieved remission at the end of the 4-week study.†11
The short-term (one-month) fixed dosing study in adults under 65 years of age demonstrated clinically meaningful (not statistically significant) reductions in depressive symptoms at 28 days for either 54 mg or 84 mg esketamine nasal spray and oral antidepressant compared to oral antidepressant and placebo nasal spray. Approximately 54 percent and 53 percent of patients treated with 56 mg and 84 mg esketamine nasal spray, respectively, responded to treatment. Approximately 36 percent and 38 percent of patients treated with 56 mg and 84 mg esketamine nasal spray, respectively, achieved remission at the end of the 4-week study.†13
The short-term (one-month) flexible dosing study in elderly adults over 65 years of age demonstrated clinically meaningful (not statistically significant) reductions in depressive symptoms at 28 days for esketamine nasal spray and oral antidepressant compared to oral antidepressant and placebo nasal spray. Of all esketamine nasal spray-treated patients, 27 percent responded to treatment and approximately 17 percent achieved remission at the end of the 4-week study.†12
Continued treatment with esketamine nasal spray plus an oral antidepressant reduced the risk of relapse by 70 percent among patients with stable response and by 51 percent in patients in stable remission, compared to continuing treatment with an oral antidepressant alone.†14
Across the five phase III and one phase II clinical trials, esketamine nasal spray demonstrated a favourable benefit-risk profile, with sustained efficacy and no new safety concerns when observed over a period of up to 52 weeks.11—,12,13,14,15 The most commonly observed adverse events in TRD patients treated with esketamine nasal spray were dizziness, nausea, dissociation, headache, somnolence, vertigo, dysgeusia, hypoaesthesia, and vomiting.11—[xvi] These side effects were generally mild-to-moderate, transient (resolving within 2 hours) and occurred on the day of dosing.
Esketamine nasal spray is a controlled drug which is intended to be self-administered by the patient under the direct supervision of a healthcare professional. Risk of harm and abuse is minimised through; safe storage, a single-use disposable nasal spray device, which prevents multi-use and safeguards against more than one dose of the drug being delivered in a single administration, and patient risk for abuse or misuse is assessed before administration. A treatment session consists of nasal administration of esketamine nasal spray and a post-administration observation period. Both administration and post-administration observation of esketamine nasal spray should be carried out in an appropriate clinical setting.
†The analysis used to calculate the primary efficacy endpoint in the acute Phase 3 clinical trial publications is the Mixed Model for Repeated Measurements (MMRM) analysis. As per the request of the European Medicines Agency (EMA), the European SPRAVATO®▼ Summary of Product Characteristics (SmPC) uses an analysis of covariance – best observation carried forward (AVCOVA BOCF). Both the MMRM and the AVCOVA BOCF are appropriate methods for analysing the change in depressive symptoms from baseline on the Montgomery–Åsberg Depression Rating Scale (MADRS). The methods yield slightly different results, but do not change the statistical significance of the study results.
In addition, response and remission rates at day 28 in the publications were calculated using patients who completed the double-blind induction period; response and remission rates in the SmPC were calculated using all patients who were randomised.16
*Professor Allan Young is a paid consultant for Janssen. He has not been compensated for any media work.
[v] Alonso, J et al. (2004) Prevalence of mental disorders in Europe: results from the European study of the epidemiology of mental disorders (ESEMeD) project. Acta Psychiatr Scand;109:21-7.
[vi] Blumenthal JA, et al. (2007) Exercise and pharmacotherapy in the treatment of major depressive disorder. Psychosom Med;69(7):587-96.
[vii] Üstün, T., & Kessler, R. (2002) Global burden of depressive disorders: The issue of duration. British Journal of Psychiatry;181(3):181-183.
[viii] Trivedi MH, et al. (2004) The Link Between Depression and Physical Symptoms. Prim Care Companion J Clin Psychiatry;6(Suppl 1):12-16.
[x] Woo J, et al. (2011) Impact of depression on work productivity and its improvement after outpatient treatment with antidepressants. Value Health;14(4):475-82.
[xi] Popova V, et al. (2019) Efficacy and Safety of Flexibly Dosed Esketamine Nasal Spray Combined With a Newly Initiated Oral Antidepressant in Treatment-Resistant Depression: A Randomized Double-Blind Active-Controlled Study. Am J Psychiatry;176(6):428-43.
[xii] Ochs-Ross R, Daly E, Zhang Y, et al. Efficacy and safety of esketamine nasal spray plus an oral antidepressant
in elderly patients with treatment-resistant depression. Poster W27 presented at ASCP 2018, 19 May–01 June,
Miami, Florida.
[xiii] Fedgchin M, et al. (2019) Efficacy and Safety of Fixed-Dose Esketamine Nasal Spray Combined With a New Oral
Antidepressant in Treatment-Resistant Depression: Results of a Randomized, Double-Blind, Active-Controlled
Study (TRANSFORM-1). Int J neuropsychopharmacol;22(10):616-630.
[xiv] Daly E et al. (2019) Efficacy of Esketamine Nasal Spray Plus Oral Antidepressant Treatment for Relapse Prevention
in Patients With Treatment-Resistant Depression: A Randomized Clinical Trial. JAMA Psychiatry. doi: 10.1001/
jamapsychiatry.2019.1189. [Epub ahead of print]
[xv] Wajs E, Alusio L, Morrison R, et al. (2018) Poster T67 – Long-Term Safety of Esketamine Nasal Spray Plus Oral
Antidepressant in Patients with Treatment-Resistant Depression: Phase 3, Open-Label, Safety and Efficacy Study
(SUSTAIN-2). Presented at ASCP 2018, 29 May–01 June, Miami, Florida.
[xvii] Lener MS, Kadriu B and Zarate Jr C. (2017) Ketamine and Beyond: Investigations into the potential of glutamatergic agents to treat depression. Drugs; 77:381-401.
[xxii] American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing.
[xxiii] Shah AJ, et al. (2010) Psychological Distress in Carers of People with Mental Disorders. BJMP;3(3):a327.
[xxiv] Al-Harbi KS. (2012) Treatment-resistant depression: therapeutic trends, challenges and future
directions. Patient Pref Adherence;6:369–388.
[xxv] Habert J et al. (2016) Functional Recovery in Major Depressive Disorder: Focus on Early Optimized Treatment. Prim Care Companion CNS Disord; 18(5).
[xxvi] Knoth RL et al. (2010) Effect of inadequate response to treatment in patients with depression. Am J Manag Care; 16:e188-96
[xxvii] Johnston K et al. (2019) The burden of treatment-resistant depression: A systematic review of the economic and quality of life literature. J Affect Disord;242:195-210.
[xxx] Mrazek, D et al. (2014) A Review of the Clinical, Economic, and Societal Burden of Treatment-Resistant Depression: 1996–2013. Psychiatr Serv;65(8):977-87.
Fampridine shown to be clinically effective when compared to best supportive care, with patients reporting significant improvement in walking ability and quality of life1
Maidenhead, UK. – Wednesday 18th December 2019 – Biogen Inc. (Nasdaq: BIIB) today announced that Fampyra® (fampridine) has been recommended for funding by the All Wales Medicines Strategy Group (AWMSG). The recommendation released by the AWMSG states that ‘Fampridine (Fampyra®) is recommended as an option for use within NHS Wales for the improvement of walking in adult patients with multiple sclerosis with walking disability (Expanded Disability Status Scale [EDSS] 4 to 7). This recommendation applies only in circumstances where the approved Wales Patient Access Scheme (WPAS) is utilised or where the list/contract price is equivalent or lower than the WPAS price.’1
Fampridine is recommended for use in all subtypes of MS, including relapsing remitting MS (RRMS), secondary progressive MS (SPMS), primary progressive MS (PPMS), and progressive relapsing MS (PRMS) that have either very limited or no treatment options, depending on disease severity.2 Wales is the first country in the UK to recommend fampridine receives funding, the Scottish Medicines Consortia are due to review their funding decision in March 2020.
“Although disease-modifying therapies have been shown to be effective in reducing relapse rates and disease progression in people with relapsing remitting MS, they do not specifically target the symptoms of MS, like problems with walking and general mobility, which can have a significant impact on quality of life,” said Dr. Simon Beck, Medical Director, Biogen UK & Ireland. “Two out of every three patients with MS will develop a degree of disability and walking impairment2, for which fampridine is licensed, making the AWMSG’s recommendation an important step forward for people in Wales who have, until now, been self-funding their own treatment.”
Fampridine’s approval came as a result of an extensive clinical trial programme; a phase II study (MOBILE) and three phase III studies (MS-F203, MS-F204 and the ENHANCE clinical trial). All studies have shown that a higher proportion of patients treated with fampridine met the response criteria (using 25-foot walking test and/or MSWS-12 end-points) compared to those treated with best supportive care.3, 4, 5 Patients responding to fampridine noted substantial improvements in routine day-to-day functional activities including, for example, the ability to walk independently without the use of sticks or any other aid for a sufficiently long enough time to manage daily tasks, with further real-world data confirming the importance of such benefits.2, 3, 4, 5 Fampridine is also a cost-effective medicine.
Ireland granted reimbursement of fampridine in September 2015 along with 12 other countries in Europe.
References
1 All Wales Medicines Strategy Group Final Appraisal Recommendation – 1919: Fampridine (Fampyra®) 10 mg prolonged-release December 2019
2 Executive summary of fampridine reimbursement submission
3Prolonged-release fampridine and walking and balance in MS: randomized controlled MOBILE trial. Hupperts R et al. 2015.
4 Long-term safety and efficacy of dalfampridine for walking impairment in patients with multiple sclerosis: Results of open-label extensions of two Phase 3 clinical trials. Goodman A et el. 2015.
5Assessment of Clinically Meaningful Improvements in Self‑Reported Walking Ability in Participants with Multiple Sclerosis: Results from the Randomized, Double‑Blind, Phase III ENHANCE Trial of Prolonged‑Release Fampridine. Hobart J et al. 2018.
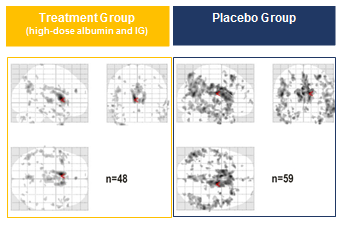
On December 6, 2019 Grifols, producer of plasma-derived medicines, concluded more than a year of encouraging results of its AMBAR (Alzheimer Management by Albumin Replacement) clinical trial with the presentation of new neuroimaging data that show the reduction in the progression of the disease in patients with mild-to-moderate Alzheimer’s disease.
These findings, released at the Clinical Trials on Alzheimer’s Disease (CTAD) Conference 2019 in San Diego, Calif. (USA), strengthen Grifols’ investigative approach using Plasma Protein Replacement Therapies.
The neuroimaging, which was measured by the FDG-PET1 technique, shows positive results particularly in patients receiving both albumin and immunoglobulin (IG). In comparison with the placebo group, these patients had less reduction of brain glucose metabolism over the 14 months of the clinical trial. This suggests that neuronal damage was reduced in these patients (see figure).
Changes in brain glucose metabolism in patients treated with high-dose albumin and immunoglobulin (IG) [right] versus placebo [left].
The images display the extension and distribution of the dark spots that relate to the reduction of glucose metabolism in the brain. Fewer and lighter spots suggest less neuronal damage, which is observed in the patients receiving both albumin and IG compared with placebo.
Grifols presented the first AMBAR results at the 11th CTAD Conference in Barcelona in October 2018. The primary efficacy endpoints, the ADAS-Cog2 and ADCS-ADL3 scales, showed a 61% reduction in disease progression for both measures in the cohort of patients with moderate Alzheimer’s.
Additional data covering the secondary endpoints of the study, such as memory and language, were presented at the 14th International Conference on Alzheimer’s and Parkinson’s Diseases (AD/PD) in Lisbon (Portugal) in March 2019, and showed a positive impact in both mild and moderate patients.
Results of other relevant endpoints, CDR-Sb4 and ADCS-CGIC5, evaluating both functional and cognitive capacity, were presented at the Alzheimer’s Association International Conference (AAIC) 2019 in Los Angeles, Calif. (USA) in July, and also pointed in the same direction when considering all treated patients together.
The CDR-Sb scale – which assesses memory, orientation, judgment, community affairs, home and hobbies, and personal care – showed a 71% reduction in clinical decline with respect to placebo in patients treated as a whole and in all three clinical trial treatment arms analysed separately.
For the ADCS-CGIC scale – which assesses several domains of cognition, daily functioning and behavior from both the patient and the caregiver perspective – a stabilisation was observed in all treated patients with respect to placebo. This effect remained in all three clinical trial treatment arms when analysed separately.
The AMBAR trial’s results are encouraging news for mild-to-moderate Alzheimer’s patients. These findings are the consequence of 15 years of rigorous scientific research at Grifols and the company will continue investigating this devastating condition that affects millions of patients around the world Dr. Antonio Páez, Medical Director of the AMBAR Clinical Program at Grifols.
Grifols will soon meet with the FDA to discuss the AMBAR clinical development program and the design of a successive AMBAR II trial that will deepen and complement the just-concluded one.
About AMBAR
AMBAR is an international, multicenter, randomised, double-blind, placebo-controlled, with parallel assignment clinical trial that enrolled patients with mild and moderate Alzheimer’s from 41 treatment centers in Spain and the United States. The study was designed to evaluate the efficacy and safety of short-term plasma exchange followed by long-term plasmapheresis with infusion of albumin combined with intravenous immunoglobulin in patients with mild and moderate Alzheimer’s disease.
AMBAR was designed to evaluate whether the progression of Alzheimer’s could be stabilised through therapeutic plasma exchange, a process that entails periodically extracting plasma and infusing albumin solution (Albutein®) with or without intravenous immunoglobulin (Flebogamma® DIF).
AMBAR targets a multimodal approach to the management of the disease based on the hypothesis that most of the amyloid-beta protein – one of the proteins accumulated in the brains of Alzheimer’s patients – is bound to albumin and circulates in plasma. Extracting this plasma may flush amyloid-beta peptide from the brain into the plasma, thus limiting the disease’s impact on the patient’s cognitive functions. Additionally, albumin has binding capacity and antioxidant properties, and both albumin and immunoglobulin display immunomodulatory and anti-inflammatory properties.
The AMBAR study included 496 mild and moderate Alzheimer’s patients, 55-85 years-old, randomised in three treatment groups and one control (placebo) group. An independent contract research organisation (CRO) oversaw the trial’s clinical monitoring phase and managed the data collection and analysis stages. The trial employed a randomised and double-blind design, meaning that neither patients nor evaluators knew whether subjects were receiving the treatment or the placebo.
The company began its research on Alzheimer’s disease in 2004 with several preclinical trials, two pilot studies and a Phase II clinical trial before launching the AMBAR trial.
Fundació ACE in Barcelona, Spain, and the Alzheimer Research Center of the University of Pittsburgh, PA, USA, have been instrumental partners in the AMBAR research and in Grifols Alzheimer’s programme since its initiation in 2004.
For more information on the AMBAR study and the results presented visit ambar.grifols.com
Those of us in the room have the power we need to fundamentally improve the quality of multiple sclerosis (MS) care in the UK, reduce variation and offer consistent care at the level we want everywhere, in the next 3 years.
In July, 85% of 120 healthcare professionals agreed with this statement (‘Raising the Bar’, MS Academy, 2019).
There are many ways to try and change healthcare, whether it is by influencing the policy-makers, collaborating with commissioners, or making clear business cases to management. However, the changes needed are often too nuanced, condition-specific, or have a return of investment too far in the future to gain the necessary attention in these circles. It can be difficult to gather the impetus needed for change to really be felt by those people directly experiencing the services. In order to effect real change in health services, often that change must be led by those delivering the services on the ground.
Navigating the landscape of service provision to meet the changing needs of a local population is challenging, and the overwhelming view of the task ahead can sometimes be too daunting to begin. As those challenges continue, they can see increasingly unsurmountable – something Jerry Clough of OPTUM describes as the ‘catch 22’.
Professor Gavin Giovannoni, chair of the ‘Raising the Bar for MS’ steering group, encouraged clinicians at ‘Raising the Bar’ (2019) saying: ‘If we break down everything we can think of that goes into MS care and improve it by 1% we can make a huge difference to MS as a whole’.
However, whilst many healthcare professionals want to be part of this 1% improvement goal locally, they often feel unequipped to lead that change, or are unsure of how to begin.
The Leadership MasterClass
Recognising this critical training gap, MS Academy has launched a 6-month multifaceted leadership programme tailored to MS experts. ‘Leadership is, simply put, influencing someone for the common good’, said Professor Gabriele de Luca, a clinician-scientist in Clinical Neurology at Oxford who has developed the new Leadership MasterClass alongside Barbara Hoese, President of Pentecore Coaching LLC.
The MasterClass will:
Identify and develop future leaders from the MS field who have little leadership experience
Develop and implement a mentoring program between participants and established leaders
Enhance skills of those who have already assumed or are about to assume leadership roles within their Institutions, the MS field, and, more broadly, the field of neurology
Leadership has lately become far more in favour than ‘management’ and the concept of effective leadership in the workplace is commonly understood. So how is leading for change different? Gabriele and Barbara note three rules, or principles, of change leadership: Change is constant, takes energy and requires coalitions.
Within the Leadership MasterClass, attendees will consider a range of concepts over the six-month programme, through face-to-face retreats, learning calls and a group project:
Leading oneself, and building effective relationships (fig 1)
Leading in a VUCA world (VUCA: ‘volatile, uncertain, complex, ambiguous’)
Negotiation, navigating conflict and performance management
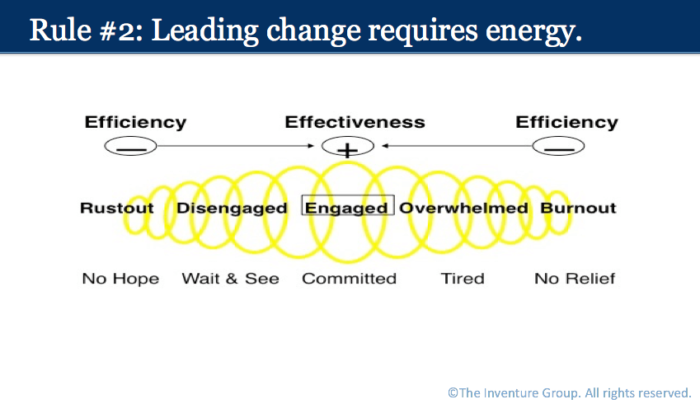
Managing personal energy to lead change (fig 2)
Figure 1: Form and self – leading from within. Effective change requires authenticity and integrity – aligning of your essence (who you are) and your form (what you do)
Figure 2: With change, leaders need people to ‘get on board’ and devote their energy to implementing change. Effective leadership requires awareness of the energy continuum in colleagues to maximise their potential.
This energy continuum (fig 2) applies to the individuals going through the change as much as the leaders themselves. Gabriele noted that ‘altering 5-8% of a person’s job can make them feel like their whole role has changed.’ As a leader, assessing the impact of the change and peoples’ attitudes towards it, and helping a team cope with the change by ‘stewarding the constants’ – noticing and encouraging the things that work well as they are and do not need to alter – is key.
‘Change starts with us’
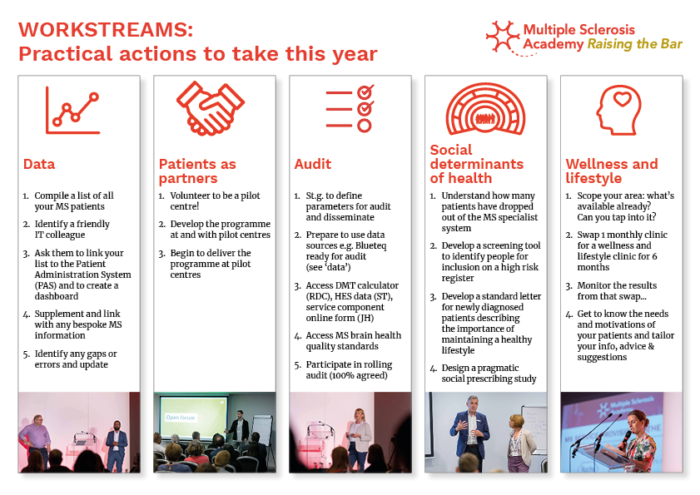
This entire leadership programme has come about because of the national drive to tackle unwarranted variation in MS services – a drive itself led by clinicians and those delivering care on the ground. When the subject of variation in UK services for MS was first broached in 2018, the take home messages from the opening event were: ‘change starts with us’ and ‘we need to do things differently’. Having developed a three-year plan across five workstreams (fig 3), the aim is that every local MS centre or service seeks to advance that plan in their area. Supporting clinical leadership through this MasterClass, sharing best practice, mentoring and peer support was seen as a key enabler to bringing the ambitious plan to fruition.
Figure 3: The five workstreams and their goals this year, each moving towards the ultimate vision: ‘To improve MS services for all people with MS and their families, and to make delivering these services for all involved a rich and rewarding experience.’
The Leadership MasterClass is selective, with each course supporting just eight delegates, and at present it is prioritising leaders in MS service provision. However, with the changing healthscape and the growing number of people living with long-term or neurological conditions coinciding with an increasingly aging population, there is no doubt that ‘doing things differently’ and ‘leading for change’ from the ground up will be essential components of our NHS going forward.
Neurology Academy is committed to supporting our healthcare professionals to deliver the services that people living with neurological conditions need to live the life they want. This is one way of doing that, and they hope to replicate the course for clinicians from other disease backgrounds in the future.
Find out more about the MasterClass and the background to both its creation and the wider ‘Raising the bar for MS’ programme at http://www.multiplesclerosisacademy.org
MAVENCLAD® (cladribine tablets) receives updated NICE guidance without full reappraisal
Update follows concerns raised by the Accelerated Access Collaborative (AAC) and NHS England that previous guidance was restricting access
Gadolinium-based MRI scanning no longer required prior to prescribing cladribine tablets for highly active multiple sclerosis
Merck announced on November 25th that the National Institute for Health and Care Excellence (NICE) has updated the Technology Appraisal Guidance (TAG) for the use of MAVENCLAD® (cladribine tablets). Cladribine tablets can now be used as an option for treating highly active multiple sclerosis (MS) in adults without the requirement of a gadolinium-enhanced MRI scan.
“Since the positive NICE recommendation for cladribine tablets in November 2017, uptake and access for first line use has been restricted due to the requirement for a gadolinium-enhanced MRI. As well as historical safety concerns about gadolinium, the areas of enhancement are transient and if the lesion is no longer visible then the patient is ineligible for treatment,” commented Belinda Byrne, Merck UK & Ireland Medical Director. “By working in partnership with the Accelerated Access Collaborative (AAC), NHS England and NICE we are delighted that we’ve been able to address this key barrier and help ensure all eligible MS patients in the UK can benefit from this innovative medicine.”
The AAC is a cross government-industry collaboration working to make the UK one of the most pro-innovation healthcare systems in the world. The AAC brings industry, government and the NHS together to remove barriers to uptake of innovations, so that NHS patients have faster access to innovations that can transform care.1
In September 2018, the AAC identified 12 ‘rapid uptake products’ already available within the UK system. These products have the potential to improve the lives of 500,000 people and save the NHS up to £30 million,2 with one of these treatments being cladribine tablets for treating highly active MS in adults.1 The AAC and NHS England promptly raised concerns to NICE that the requirement in the guidance for gadolinium-enhancing MRI prior to treatment was restricting access to cladribine.
“Cladribine has been selected by the Accelerated Access Collaborative (AAC) as a rapid uptake product due to the clear benefits it offers for both MS patients and the UK healthcare system. The gadolinium-enhanced MRI requirement in the previous NICE guidance was a significant barrier for many clinicians and their patients,” said Dr Waqar Rashid, consultant neurologist at St George’s University Hospitals Trust. He continued,
We are extremely pleased that NICE has revised its guidance after feedback from NHS England and the ACC, and that this innovative medicine will now be more rapidly and widely available to patients with highly active MS.
David Martin, Chief Executive Officer of the Multiple Sclerosis Trust added, “We are very pleased that NICE have amended criteria for access to Mavenclad. Now people with MS face one less barrier to accessing an effective MS treatment.”
Cladribine tablets are a short-course oral treatment available in the UK for adults with highly active relapsing MS, that can help reduce relapses for up to four years with a maximum of 20 days’ oral treatment, taken in the first and second year.3,4 Following completion of treatment in the first two years, no additional treatment is required in years 3 and 4.5
The manifesto has been published in response to current threats and challenges to credible research across life sciences. Currently, there is a huge pressure to publish as many papers as possible, with an emphasis on dramatic, novel findings. This in turn has led to increasing levels of non-reproducible research[i], which can skew scientific understanding, contribute to hyped expectations, and jeopardise the translation of research to real-world applications.
At the BNA, we recognise our responsibility to directly address these issues within neuroscience, and as a result, we have developed a vision for change. Change that will ensure that neuroscience research is as robust, reliable, replicable and reproducible as possible; in short, to ensure the credibility of neuroscience.
To achieve this, our manifesto outlines three commitments:
Supporting a shift in research culture that’s welcomed and desired by the whole neuroscience community.
Equipping all neuroscientists – regardless of career stage, location, research topic or specialist technique – with the skills, knowledge, tools and processes they need to carry out neuroscience research which is as credible as possible.
Changing the landscape in which neuroscientists operate, so that the influences which drive neuroscience research also drive the most credible research.
To ensure a sustainable future for 21st century neuroscience research, we must ensure the credibility of research – that it is reproducible, replicable, and reliable. That means rewarding the best science – science which lays equal value on both positive and null outcomes, that recognises the importance of reproducibility or replication, and can sometimes be slow to progress. But be reassured, this isn’t a campaign of saying and sermonising – this is one of doing. From sharing best practice and creating a space for vigorous discussion and debate, to equipping researchers with the right tools and incentives to try something new. We are committed to supporting everyone to make changes and embrace new practices, in order to advance and secure the future of neuroscience.
Chief Executive, Anne Cooke also commented:
As neuroscientists, we have a duty to strive for the best science: science that is reliable, sustainable and will make a difference to our future. Working together is key to this, engaging with everyone within the community, from journal publishers and societies, to universities, funders and the general public. As an organisation, we’re committed to working together as one neuroscience community, ensuring everyone is equipped and supported to make changes that will help achieve our vision.
Supported by The Gatsby Foundation, tonight’s event presents an exciting opportunity to raise the profile and awareness of ‘Credibility in Neuroscience’, with addresses from Professor Dorothy Bishop, Professor Lord Robert Winston, and BNA Chief Executive, Dr Anne Cooke.
About ‘Credibility in Neuroscience’
The BNA’s campaign, ‘Credibility in Neuroscience’, is one of our most important programmes to date, to drive open, transparent and reproducible research.
The programme champions the principles of open science, replicability, reliability and reproducibility in research, and challenges some aspects of today’s research environment – such as ‘publish or perish’ – which can have a counter-productive and damaging effect.
Sign up to receive our email newsletter with links to the latest content. ACNR is free, thanks to the support of advertisers. The editorial content is peer reviewed and remains completely independent unless clearly specified.