11th April 2017 was World Parkinson’s Day and the anniversary of James Parkinson’s birth. It was also 200 years since he published his essay on the shaking palsy.
Watch our film about world authority on PD Professor Andrew Lees, by award winning documentary maker Ben Crowe, in which Professor Lees calls for a more creative approach to research.
Teva Pharmaceutical Industries Ltd have announced that the label for COPAXONE® (glatiramer acetate) injection 20mg/mL, used for treatment in patients with relapsing forms of multiple sclerosis (RMS), has been updated in the UK to remove the pregnancy contraindication.
The label update followed an extensive analysis by regulatory authorities of available pregnancy cases among women who were already taking COPAXONE® when they learned they were pregnant. A supporting analysis was also provided comparing data from Teva’s Glatiramer Acetate (GA) Pharmacovigilance Database which captured more than 8,000 pregnancies over a period of more than 20 years.
Staying on an MS treatment like COPAXONE® 20 mg/mL is now an option women can discuss with their doctor because COPAXONE® is no longer contraindicated during pregnancy.
As a precautionary measure, it is preferable to avoid the use of COPAXONE® during pregnancy unless the benefit to the mother outweighs the risk to the foetus.
Professor Gavin Giovannoni, Chair of Neurology – Blizard Institute, Barts and The London, said, “People with multiple sclerosis want to live normal lives, but, for many women with relapsing MS, having to decide between planning a family and staying on their treatment to manage relapses is a reality they have to face. This label update provides specialists and their patients with MS, who are considering starting or extending their family, an important option in relation to their treatment of MS during pregnancy.”
The European Commission (EC) has extended the Marketing Authorisation for Zebinix® (eslicarbazepine acetate) as a once-daily adjunctive treatment for patients aged above six years with partial-onset (focal) seizures with or without secondary generalisation.[i]
Eslicarbazepine acetate was previously indicated only for the adjunctive treatment of adults aged over 18 with partial-onset seizures with or without secondary generalisation.[ii]
The variation to the license is based on data from one Phase III study (305), one Phase II study (208) and from population PK modelling and exposure-efficacy analyses. The Commission considered the efficacy results from the mentioned studies to be acceptable for an extension of the Marketing Authorisation. The safety analyses show no new or unexpected safety ndings and eslicarbazepine acetate does not appear to have negative neurocognitive consequences (power of attention, information processing and working memory).[iii]
This is an edited excerpt from Ross’s Story in Life After Encephalitis by Dr Ava Easton (pages 55-61). Published in 2016 by Psychology Press. Copies can be purchased from The Encephalitis Society (www.encephalitis.info) or from Amazon, among other suppliers.
Ross’s Story
Ross has been feeling unwell for some weeks now, and is being treated for depression and anxiety…
“My dad asked me to go and see his GP. It was probably the tenth visit to a GP in the space of six weeks, but I agreed. This GP prescribed beta-blockers and another anti-depressant. This would be the third anti-depressant drug I had been prescribed in six weeks. I had seen four different GP’s all of whom had different ideas about how to treat me. How did I know who to believe?
The 10th of July was a very bad day…I kept telling my family there was something wrong with me; that it couldn’t just be depression. I started hitting my head against walls to try and knock the burning out of it…I was screaming. I was crying. I was in agony. I was convinced that I was about to die. My parents called 999 and I was taken to hospital for chest x-rays and CT scans of my head. I spent the night terrified that the lumbar puncture that they were planning to do would go wrong and I would end up disabled after it. That next morning a doctor told me that there was nothing wrong with me physically, they weren’t going to do the lumbar puncture, and that I had a mental problem. I was discharged.
I returned to my parent’s home…the tingling started…it was going to happen again. I lost all sense of what was right in the world. The screaming started again…I couldn’t think, and worse, now I couldn’t remember. I couldn’t picture people’s faces in my mind. I started shouting out friends and family names as I thought that if I didn’t I was going to forget them. It literally felt as if memories were draining out of my brain. I was taken back to hospital for the second time in 24 hours…I was discharged for a second time, and the local crisis team visited daily.
Things began to feel a little more under control. I was referred to a psychologist, and I was prescribed an anti-psychotic medication. This made me very dozy but at least it controlled things.
By now I had spent months convinced that it couldn’t be a mental health problem. I had tried everything I could to make myself happy: I had reduced work, taken breaks away, but nothing was helping. Every morning I started the day questioning what the point of the day was; what the point of existing was.
I made it through the next few weeks, then something happened. Life was turning very dark. On the 26th August I was at home on my own. I took a belt, wrapped it around my neck and wedged the end in the top of a closed door. I let the belt take the weight and I was happy that it would soon be over. Fortunately the belt snapped. That night my girlfriend found out what had happened. She rang the crisis team who were close to taking me away with them, but, they didn’t.
On the 30th we were due to fly to Crete. The crisis team said even thinking about going was a bad idea. However, I was determined to try, just to keep some normality in my life. We got in the car but didn’t get far before the panic started. I was trying to get out of a moving car, and my girlfriend turned the car round and headed home. The crisis team were called again – I was placed under section two of the mental health act, and taken to hospital.
I was transferred to a higher security hospital where I remained for seven weeks. My medication was increased to keep me stable and in the October I was transferred to a general hospital, where I was scheduled to see a sleep specialist since my sleep was getting more bizarre.
The sleep specialist looked at me in a new way – in a way other doctors hadn’t. I owe him a lot, probably my life. After being with him for hours, he wrote to the mental health hospital saying I should be reassessed and probably taken off all of the drugs I was on. I was referred to a neurologist, and spent a month in the neurology ward with the consultants searching for an answer. Finally, the test for anti-NMDA receptor encephalitis returned positive. My brain was seriously unwell, and I was immediately started on Intravenous Immunoglobulin (IVIg) treatment.
The 8th of November 2014 is the first day that I remember since the middle of August. I remember lying in a bed thinking “where on earth am I?” In front of me was a notepad with a note from my mum saying I was in hospital and that it was the middle of November.
Looking back, the biggest clue to there being something wrong were my memory issues. With the depression and anxiety we kept finding possible reasons for them, but the memory loss? That was unexplainable. I started to forget pin numbers, passwords, directions, how to use maps, how to put up a tent, I couldn’t remember names or faces. The only explanation anyone provided was I was so stressed that I was just shutting down.
I don’t hold a grudge about what I went through, I just wish they had thought about, and looked for, a cause outside of their own discipline earlier on. Mental Health and Neurology both work with the brain – stronger links between the two may have saved me months of misdiagnosis.”
Submitted by: Dr Ava Easton Published online: 21/2/17
The Encephalitis Society began life in 1994 when it became clear there was little to no information or support for people affected by encephalitis and their families. Today The Society has the vision:
To live in a world where Encephalitis is as rare as it possibly can be given its eradication is unlikely, and that those affected and their families, have access to early diagnosis, excel- lent management of their condition, timely access to rehabilitation and other forms of social support.
Its primary aim is to ‘Improve the quality of life of all people affected by encephalitis’, and The Society achieves this in three primary ways:
Supporting adults and children affected by Encephalitis, their families and carers by providing advice and evidence-based information and working at a national and international level to improve services.
Raising awareness about the condition and its subsequent problems among relevant professionals, statutory agencies and the general public.
Conducting research and work in part- nership with other researchers and their establishments.
The Illness
Encephalitis is inflammation of the brain. The inflammation is caused either by an infection invading the brain (infectious); or through the immune system attacking the brain in error (post-infectious or autoimmune encephalitis). Encephalitis is a thief, one that has quietly been at work for hundreds of years, robbing families of their loved ones, and even in those families where the person survives, it often robs them of the person they once knew. Encephalitis steals their capacity to remember as well as their personalities and the types of abilities we all generally take for granted: concentration, attention, thinking, judgement, inhibition. For many there are additional outcomes such as epilepsy and levels of fatigue so great that returning to work or education are mere pipe dreams. This is of course, where the person survives, many don’t. For many years statistics around incidence were scarce to non-existent and encephalitis was side-lined into the silo of ‘rare disease’. However due to great work conducted by many committed researchers and their insti- tutions over the last decade we now know there are around 6000 people diagnosed with encephalitis in the United Kingdom alone 1 each year. That’s 16 people every day. The authors suggest this may be an underestimate. Not only that but it is thought that, and again this is an underestimate, that encephalitis is costing the NHS around £40 million a year. A gure that does not include the costs of rehabilitation, long-term care, and the loss to the economy from those of working-age unable to return to work.
Therefore encephalitis has a higher incidence than motor neurone disease and certain forms of meningitis.2 Yet, despite encephalitis being more common, these conditions continue to receive a much higher clinical and public profile. Invariably people have not heard of Encephalitis unless it has happened to them or they are caring for a survivor.
Support and Information
Support and information for survivors and family members is critical. Encephalitis is a complex condition to diagnose and manage. Therefore a lot of the information surrounding it is often complex for the uninitiated. The Society takes this information and restructures it in ways that are meaningful for those new to the condition. Information consists of factsheets, newsletters, and guides for adults and families. All the information provided is evidence-based, peer-reviewed and accredited by NHS England. Therefore patients and professionals alike can be assured about the reliability of the material. The Society also provides direct support via phone, email, skype, and chat online. Other services include connecting people in a similar situation, and a burgeoning global network of volunteers. There are also moves afoot to provide more long-term and social support to patients in evolving encephalitis clinics in Oxford and London.
More recently The Society has launched The Encephalitis Society Neuropsychology Service. This operates in the knowledge that neuropsychology is perhaps the primary intervention that, if a person survives, can help support The Society’s primary aim of improving people’s quality of life. The service is operated by a consultant Neuropsychologist and is not established to duplicate the work of the many excellent services around the country. The service is there primarily to pick up people in areas where a neuropsychology service does not exist, and also in areas where waiting lists are detrimental to maximising a person’s potential recovery and rehabilitation (http://www.encephalitis.info/support/neuropsychology-service).
Awareness
The Society’s primary awareness drive is World Encephalitis Day on 22nd February each year (http://www.worldencephalitisday.org). This global day was launched in 2014 and to date has reached more than 20 million people since its inception. 2017 sees landmark buildings and businesses around the world illuminating in red, in order to drive awareness about the condition, through digital and social media channels. There are lots of other ways each year for people to get involved by engaging with their #RED4WED and #ShowYouKnow campaigns as part of the day’s activities.
Research
The Society is involved with a plethora of research studies including two randomised control trials in Oxford and Liverpool. The Society provides a substantial amount of information for professionals each year including an ‘Advances in Research’ guide which acts as an annual archive of the year’s most prom-inent research into the condition. In addition there are a range of initiatives engaging with junior doctors and early years’ researchers such as essay prizes and travel bursaries. The Society also contributes to research financially and has just launch a co-funded PhD fellowship with The University Liverpool. There is also a popular annual conference held in December in London each year and which brings interested professionals up to speed with the latest in the condition.
The Society strives hard to meet its aims and objectives. They achieve a huge amount with few resources, a small team, and with the voluntary contributions of its Board of Trustees and Scientific Advisory Panel.
References
Granerod J, Cousens S, Davies NW, Crowcroft NS, Thomas SL. New estimates of incidence of encephalitis in England. Emerging Infectious Disease 2013;19(9).
Easton, A. Life After Encephalitis: A narrative approach (2016). Routledge. Oxon
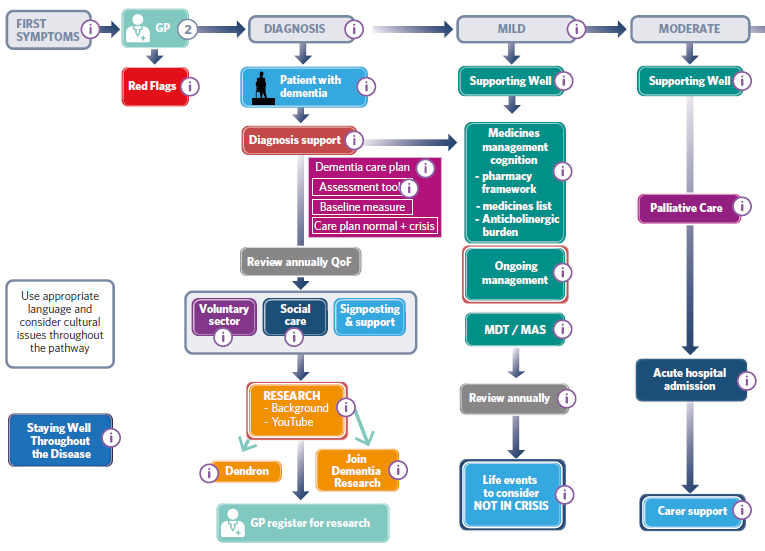
Interactive pathway toolkit provides a one-stop shop resource for professionals working in dementia care
Following a partnership between academia, the NHS and the third sector, clinicians can now access a free toolkit containing a comprehensive roadmap and resources for the care of people with dementia.
The Dementia interactive care pathway toolkit maps out the care pathway a dementia patient will follow and provides an aide-memoire for the services and support needed from diagnosis to end-of-life care.
The toolkit’s invaluable compendium of resources can be accessed via an interactive PDF which enables clinicians to easily navigate the different elements of the care pathway and access relevant documents and further information all in one place.
It helps all professionals involved in the care of people with dementia, including commissioners, to plan services, and has a particular focus on supporting patients to stay well in order to promote independence and avoid crisis.
The toolkit is the brainchild of Dementia Academy Faculty members Dr Iracema Leroi, Sue Thomas and Dr Tony Burch who worked in partnership with the University of Manchester and Greater Manchester and Eastern Cheshire Strategic Clinical Network (SCN), and with support from Wilmington Healthcare. A range of stakeholders – including people with dementia, their carers, medical professionals, police and ambulance personnel, social workers and commissioners, were also involved in the creation of the toolkit. Consequently, it reflects firsthand experiences of the challenges involved in dementia care.
Sarah Gillett, Managing Director of the Dementia Academy said:
Patients with dementia have complex needs which can be best supported when a true synergy is achieved across the different health and social care disciplines.
The toolkit is a powerful resource for supporting health professionals across the country to deliver a best practice dementia care service. We hope that it will enhance the dedicated efforts of the many people looking after people with dementia in England.
Dr Iracema Leroi, who is a Faculty member at the Dementia Academy, and Clinical Senior Lecturer Honorary Consultant in Psychiatry, University of Manchester, Manchester Mental Health and Social Care Trust Institute of Brain, Behaviour and Mental Health, said:
This pathway is a wonderful new tool to help frontline professionals support people with dementia and their carers. It’s a veritable ‘Aladdin’s cave’ of interesting bits of information and guidance about the multitude of problems which people with dementia may face.
“We intend the tool to be dynamic and flexible so that anyone using it can adapt it to their own local circumstances and update it as new evidence about better care becomes available. It can be stored on a desktop for ‘quick reference ‘ and each component can be studied in more depth as required. We are sure that it will become an invaluable part of daily practice to support people with dementia.
Faculty member Dr Tony Burch, who is a GP in NHS Brent Clinical Commissioning Group said:
There is currently huge interest in and awareness of dementia. In the last year, NHS England has focused on ensuring that two thirds of the estimated number of people with dementia will have a formal diagnosis and post diagnostic support.
To help achieve this, NHS England wants to facilitate information so GPs can feel safe about diagnosing dementia in particular clinical situations. There is a need to empower GPs to be able to make a diagnosis if they think that is clinically justified and appropriate. The new toolkit is a vital instrument to ensure GPs have the skills and confidence to do this.
The toolkit was created in partnership with the then Greater Manchester, Lancashire and South Cumbria SCN, which from April 2016 became Greater Manchester and Eastern Cheshire SCN. The SCN, which worked in particular to map the Dementia Well Pathway framework and develop accompanying best practice resources with the input of a plethora of experts, will now be promoting the toolkit across the Greater Manchester and Eastern Cheshire area.
Dementia Academy Faculty member Sue Thomas, who facilitated the creation of the toolkit through her role as CEO of Commissioning Excellence services at Wilmington Healthcare, added:
We have been delighted to facilitate the development and publication of this toolkit which adds to the wide range of integrated care pathways that are available currently.
The Dementia interactive care pathway toolkit is available to download at:
STADA Australia continues to innovate in Parkinson’s Disease with MOVAPO® pre-filled syringes (PFS)
Parkinson’s Disease is a surprisingly prevalent condition with an estimated 10 million people worldwide and roughly 70,000 Australians (1 in every 340 people) suffering from the condition.1 It is the second most prevalent neurological condition exceeded only by dementia. It is more common than some cancers including breast, colorectal, lung, ovarian, leukaemia to name a selection.1 With people living with Parkinson’s Disease for well over 20 years, it places a significant economic burden on the health care system, employees, patients and their carers.1
Parkinson’s Disease is mainly a clinical diagnosis. However, modern imaging and nuclear techniques can provide supplementary information allowing a precise distinction from differential diagnosis, such as essential tremor or other parkinsonian syndromes. It can provide a more accurate and earlier diagnosis.2
With no cure confirmed, treatments all aim to minimise a patient’s symptoms and side effects, maximise their quality of life and slow the progression of the disease. As with all medications there are benefits and risks and prescribers will evaluate all of these at each stage along the disease continuum.
Oral therapies are the first line of treatment and are effective for most patients in the early stages of the disease (first 2-3 years post the onset of signs and symptoms).3 However, long-term oral levodopa has limitations despite patients taking optimised regimens.3 Motor fluctuations are experienced by up to half of levodopa-treated Parkinson’s Disease patients by 2 years after the start of therapy3 with other studies confirming the emergence of motor complications after 4-6 years, including medically refractory fluctuations and /or dyskinesias.2 Over time, regular and/or unpredictable ‘off’ periods negatively impact patients’ daily routines and their overall quality of life.3 Delayed gastric emptying attributable to Parkinson’s Disease can affect absorption of oral medications resulting in gaps of levodopa’s benefits despite regular oral dosing. 3,4,5 Hence, alternate classes of therapy with different routes of administration may need to be considered.
A second line established approach for treating patients refractory to conventional oral drug therapy is administration of the dopaminergic agonist apomorphine. MOVAPO (apomorphine hydrochloride) pre-filled syringes (PFS) are indicated to reduce the number and severity of ‘off’ phases in patients with Parkinson’s Disease severely disabled by motor fluctuations refractory to conventional therapy. Initiation of therapy with apomorphine should be undertaken in a specialist unit in a hospital setting. Conventional therapy should be continued during ‘on’ phases.6
Continuous subcutaneous apomorphine infusions should be evaluated before more invasive measures or neurosurgical interventions are contemplated. 7
MOVAPO continuous infusion as second line treatment, has clinically proven benefits and is an effective option for patients with Parkinson’s Disease who are experiencing severe fluctuations and are poorly controlled by conventional oral therapy. 3,7,8
MOVAPO significantly reduced ‘off’ time by 40-85% vs baseline (p = 0.0003)3*
MOVAPO significantly reduced dyskinesias during ‘on’ time and reduced the severity of dyskinesias that do occur by 15- 65% vs baseline (p = 0.0003) 3,7^*
MOVAPO allowed reductions of 15-80% in levodopa doses vs baseline (p = 0.003), reducing the treatment burden for patients3*
MOVAPO on average, decreased ‘off’ time by approximately 5.5 hours per waking day vs baseline (p < 0.0001)8¥
*Bhidayasiri et al is a review article that provides an overview of the pharmacokinetic properties and efficacy of apomorphine given intermittently and as continuous infusion for patients with Parkinson’s Disease and otherwise intractable motor fluctuations as an alternative to other dopaminergic treatment.3
^Deleu et al is a comprehensive systematic review of literature from 1960 to 2004 via MEDLINE and EMBASE of subcutaneous apomorphine across its different indications in Parkinson’s disease.7
¥Ruiz et al is a retrospective study that evaluated 82 patients with Parkinson’s Disease (disease duration 14.39 years ±5.7, mean age 67 years ±11.07) and severe motor fluctuations treated long-term with continuous subcutaneous apomorphine infusion over a mean follow-up period of 19.93 months ±16.3. The mean daily dose of apomorphine was 72 mg.8
A recent innovation to the MOVAPO range is the MOVAPO® pre-filled syringe (PFS). It simplifies the administration of this medication for patients, nurses and carers.6 Doctors can confidently transition patients from MOVAPO ampoules to MOVAPO PFS.6
MOVAPO PFS provides accurate dosing – there is no requirement for mixing or diluting apomorphine
MOVAPO PFS minimises risks of injury – no ampoule breakages, no sharp needles for mixing
MOVAPO PFS reduces monthly consumables costs – no requirement for saline for dilutions
MOVAPO PFS is easy to administer – there is a simple connection between PFS and Mark II or Mark III pump
Public Hospital Prescriptions: For those prescribers initiating MOVAPO pre-filled syringes (PFS) in a public hospital a streamlined code 10950H will need to be included on all prescriptions
Private Hospital Prescriptions: Those specialists initiating MOVAPO pre-filled syringes (PFS) in a private practice or private hospital setting using an S100 Highly Specialised Drug Authority Prescription (PBS/RPBS), will need to provide Medicare Australia with the prescribing code 10971K, and the private hospital provider number.
STADA, established itself in Australia and New Zealand in 2016 with its full focus and commitment on Parkinson’s Disease, those physicians and nurses treating the disease, the patients and their carers. STADA aims to improve the lives and outcomes of patients living with disease through a variety of recently launched initiatives including:
A new variable flow rate infusion Mark III pump
A new format of MOVAPO in a pre-filled syringe improving administration
The STADA Nurse Advisor service who train prescribers, patients and carers how to administer MOVAPO PFS with the Mark II or Mark III pumps
iMOVE programme, (available from the APP Store or Google Play, computer or phone), provides patients with:
The ability to order consumables via the iMOVE shop
Access to a full suite of patient support materials, including instructions and troubleshooting guides, videos, brochures, travel letters, and more
Instant contact with the STADA Nurse Advisor Service
A simple referral tool to share with friends and carers
The STADA Wall is available via myINTERACT, and is a platform that allows healthcare professionals easy access to relevant and engaging content on smartphones or tablets and can be downloaded via the APP store or Google play. This resource provides HCPs with immediate access to the STADA Nurse Service, educational resources that can be used with patients, regulatory and reimbursement information and events and activities.
If you need additional information on MOVAPO, STADA support programmes or Parkinson’s Disease, please make contact with the most appropriate person listed below.
1. Deloitte Access Economics Report “Living with Parkinson’s Disease An updated economic analysis 2014 Parkinson’s Australia Inc”. August 2015 2. Pedrosa DJ, Timmermann L Neuropsychiatric Disease and Treatment 2013:9 321–340 3. Bhidayasiri R et al. Clin Neuropharm 2015;38:80-103 4. Merrinan S et al. Mov Disord 2014:29(1):23-32 5. Pfeiffer R et al. Parkinsonism Relat Disord 2011;17:10-15 6. MOVAPO PFS Australian Product Information 7. Deleu D et al. Drugs Aging 2004;21(11); 687-709 8. Ruiz PJG et al. Mov Disord 2008;23(8):1130–1136
For the first time in the UK, a short-film has been launched to raise awareness of the world’s most common inherited neurological condition Charcot-Marie-Tooth (CMT). It aims to spread the word about the condition because so few people have heard of it. Watch the film at http://cmt.org.uk/video/
The film has been backed by CMT expert and President of the Association of British Neurologists, Professor Mary Reilly and charity CMT UK, which supports people with CMT, a condition with a wide variety of symptoms including uncontrollable pain, chronic fatigue, unstable ankles, balance problems and falls.
The one minute film – the idea for which came from Douglas Sager (67) who found out he had CMT in 2011 – features people of various ages and at different stages of the condition including Harvey Rogers (10) who has minor nerve damage, his mother Lisa Rogers who has difficulty walking and Emma Lines who is now in a wheelchair and struggles to open a can of pop due to poor co-ordination in her hands. It is interspersed with X-ray style animation so that each person is shown as a digital body of nerves, revealing what can happen when they malfunction.
While CMT is currently incurable, early, accurate diagnosis can improve the lives of those with the condition. Charcot-Marie-Tooth is named after the three scientists who discovered it. Steadily progressive, it causes muscle weakness in the lower legs and hands, leading to problems like hammer toes, restricted mobility, uncontrollable pain and carrying out tasks needing fine motor skills, such as fastening shoe laces. However, people with CMT have a reasonable quality of life with normal life expectancy.
CMT UK’s chief operating officer, Karen Butcher said: “Douglas fundraised for this film off his own back and we are delighted with the end result, which is compelling, human and informative. There is so much to tell people about CMT but this captures the bones of it well.”
The CMT awareness campaign is being backed by medical professionals including Professor Mary Reilly.
The film was written, produced and directed by award winning film maker and director, Tim Partridge and also has the backing of Shadow Foreign Minister, Catherine West MP.
Catherine said: “I first met Douglas when he came to my constituency surgery and told me about Charcot-Marie-Tooth disease, its problems and lack of awareness about it. It was wonderful to launch the film in Parliament and I hope that it will lead to greater awareness of the cause and symptoms not only in the UK but throughout the world”.
Conference details: 14-17 September, 2016; London, UK News source: ECTRIMS congress organisers, and company press releases First published online: 13/10/16
ECTRIMS and EAN join forces to formulate the first European MS treatment guidelines
The Clinical Guideline on the pharmacological management of people with Multiple Sclerosis was developed jointly by ECTRIMS and European Academy of Neurology (EAN).
This is the largest European collaboration to consider therapeutic guidelines for MS and have been developed following the GRADE methodology that implies a sequential assessment of the quality of evidence, followed by judgment about the balance between desirable and undesirable effects, and subsequent decision about the strength of a recommendation. The main recommendations presented by Susana Otero (Multiple Sclerosis Center of Catalonia, Barcelona, Spain) are based on the latest evidence available worldwide and have been agreed by a large working group of key MS experts across Europe, as well as patient representatives from MS advocacy groups, such as EMSP and MSIF.
New guidelines for patients with clinically isolated syndrome
One of the key consensus statements which came out of the recent ECTRIMS/EAN meeting concerns patients with clinically isolated syndrome. These are patients that have had only one neurological incident and do not fulfil current diagnostic criteria for MS.
Based on the available evidence and mindful that MS is a progressive disease and delay in starting disease modifying treatments can have long-term consequences, the steering committee has recommended that CIS patients with visible abnormalities on MRI scans should receive disease modifying drugs (DMD) prior to diagnosis.
Consensus on treating patients with established MS
Research advances in recent decades mean that clinicians now have a large choice of effective drugs for the treatment of patient with confirmed MS. However, few of those drugs have been compared directly and the trial populations are too heterogeneous to draw direct comparisons.
The ECTRIMS/EAN steering group have therefore recommended that choosing the right drug for an individual patients with established MS should remain in the hands of the treating neurologist taking into account the patient’s history, their age, their level of disease activity, their comorbidities and, very importantly, their personal preferences. Drug choices may also depend on availability within different healthcare systems and different licencing regulations across Europe.
The experts within the committee hope that on-going and future trials may provide further clarity and recommendations will be made as time goes on, when the evidence on which to base them becomes available.
Guidelines on monitoring the effectiveness of MS treatments
The steering group did agree that regardless of the drug chosen, regular monitoring should take place to investigate whether that treatment is having an impact on the disease.
The timing of monitoring will depend on many factors and will differ between countries but the ideal is for patients to have an MRI scan about 12 months after starting a drug treatment. If there is a poor treatment response, then the treatment strategy should be to move on to a more aggressive drug
Susana Otero, Multiple Sclerosis Center of Catalonia, Barcelona, Spain
Guidelines for treating patients with Primary Progressive MS (PPMS)
PPMS is diagnosed in around 10-15% of MS patients and currently has no disease modifying pharmacological treatment. Ocrelizumab, a potential treatment for PPMS, has recently be tested in a phase 3 clinical trial and results have been very encouraging, but the drug is currently still under review by the European Medicines Agency.
The ECTRIMS/EAN steering group has recommended that PPMS patients should receive Ocrelizumab and this consensus statement will be included in the published guideline – but only if the drug is licenced before the publication date, explains Otero.
ECF Satellite Symposium at ECTRIMS attended by 1600 MS professionals
The European Charcot Foundation welcomed more than 1600 MS professionals at its Satellite Symposium held during the congress.
The symposium “the role of B-cells in MS pathogenesis” chaired by Prof. Giancarlo Comi, addressed the following topics:
1.Why antibody therapy in MS (Prof. H.P. Hartung – Germany)
2.Update of the role of b-cells follicles in MS (Prof. R. Reynolds – UK)
3.Anti b-cells therapy in MS and related disorders (Prof. G. Comi – Italy)
Global research is focusing on better therapies for all stages of multiple sclerosis
The final late-breaking session session at ECTRIMS included news on the progress that is being made in determining the most effective drug treatments for the relapsing remitting stage of MS and in developing much-needed novel therapies for the secondary, progressive stage.
Alemtuzumab: using real world clinical data to find out how it compares to other MS drugs
One of the key presentations reported important results comparing alemtuzumab with beta interferon, fingolimod and natalizumab. All four drugs are licensed for the treatment of patients in the relapsing-remitting stage of MS, in which episodes of new neurological symptoms are followed by at least partial recovery.
Research over the last two decades has revolutionised therapy for MS patients and disease-modifying drugs are now often used as soon as a diagnosis is made in order to slow disease progression and delay the onset of disability.
New drugs have been developed regularly and individual treatments have been licensed when they have proved effective compared with placebo or one established treatment. A new drug does not need to be tested against all available treatments for MS, so the efficacy of already licensed drugs is difficult to compare. A comparison over different clinical trials is compromised by the fact that individual trials may differ significantly in their design and may be undertaken in very different groups of people.
The answer to this problem is to gather data on how all these drugs perform after they are approved for use in the clinic. MSBase (https://www.msbase.org) is a registry that aims to collect clinical outcome data from people with MS in real-world clinical practice. By collecting sufficiently large amounts of such data, it is possible to statistically match the different patient populations and allows comparing the efficacy of different treatments in routine clinical practice.
Tomas Kalincik (University of Melbourne, Australia), on behalf of the MSBase collaboration, presented results from a study comparing the efficacy of alemtuzumab against three other treatments (fingolimod, beta interferon and natalizumab), all of which have been shown previously to reduce the frequency of MS relapses.
The real world data confirmed trial results and showed that alemtuzumab was better at suppressing relapses compared to beta interferon and fingolimod, and was similarly effective compared to natalizumab. Although patients treated with natalizumab showed slightly more clinical improvement than those treated with alemtuzumab, the rates of disability progression did not appear to differ significantly between the two drugs.
These findings demonstrate that real-world data obtained as part of clinical practice can be used to answer questions about the relative efficacy of treatments that would be difficult and prohibitively expensive to answer in dedicated treatment trials. This is important for people with MS, and the clinicians who advise them, to enable well-informed choices between treatments based on their relative efficacy and the risk of side effects.
More news about new treatments for secondary progressive MS
During the late break session, details were given about the EXPAND trial of the novel therapy siponimod (BAF312).
Many people with MS who have initially had relapses and remission eventually develop progressive disability that is not the result of relapses. This is known as secondary progressive MS (SPMS) and currently licensed treatments have only very moderate efficacy.
In the late breaking news session, Ludwig Kappos (University of Basel, Switzerland) reported the main results of EXPAND, which has included 1,651 patients with SPMS from 31 countries. SPMS patients, who were included only if they showed evidence of disability progression within the previous two years, were treated daily with either 2mg siponimod or a placebo (two patients were placed in the treatment group for every one patient in the placebo group).
The main outcome was confirmed MS progression over three months, measured using Expanded Disability Status Scale (EDSS) scores. When compared with placebo, siponimod reduced progression by 21% (HR 0.74), and this difference was statistically significant. At 6 months the reduction was 26%, and again this was statistically significant. Treatment effects were more noticeable in those who had had relapses, and treatment was associated with a reduction in the annualised relapse rate (which fell by about half compared with the placebo group).
The take home message from today is that EXPAND is the largest study to date to present data showing that a drug candidate for secondary progressive MS (siponimod) impacts on a clinical measure of disability progression. It is encouraging that we now have a potential treatment for SPMS that might be available for patients in the near future.
Prof. Xavier Montalban, President of the European Committee for Treatment and Research In Multiple Sclerosis
Refining the criteria used to diagnose MS at an early stage using MRI scan results
Presentation revealed the latest evidence-based thinking on how to use MRI scan results to diagnose MS with increasing accuracy.
Earlier this year, MAGNIMS, the European Collaborative Research Network that studies the use of MRI when diagnosing MS, published revised criteria for clinicians.
In his presentation at ECTRIMS, Paolo Preziosa (Vita-Salute San Raffaele University, Milan, Italy) a young investigator within MAGNIMS, outlined results showing that their most recent techniques do indeed make it possible to diagnose MS earlier and more accurately in patients with very few clinical signs of the disease.
Using MRI data in MS diagnosis requires continual reassessment
MRI scans have been used routinely to help diagnose MS since 2001. Over the last 15 years there have been huge advances in the technology and so the criteria used to diagnose MS in patients on the basis of their scans results have had to change too.
One of the key goals is to use MRI imaging to detect changes within the brain and spinal cord of someone who has Clinically Isolated Syndrome (CIS). This term is used to describe someone who has experienced a single episode of neurological symptoms. This episode may have lasted only a few days, leaving clinicians with very little to go on when attempting to determine the underlying cause.
One of the key factors that MRI data is used to look for is whether the symptoms are caused by lesions in the nervous system that are ‘disseminated in time and space’. Using MRI technology to judge whether abnormalities in the grey matter particularly are associated with a subtle spread and progression of the disease is at the heart of the recent criteria.
Defining the criteria for a diagnosis of MS
Preziosa explained that the new criteria for MS diagnosis in patients with CIS specify that at least two of the following signs are visible on a detailed MRI scan:
At least one lesion in the spinal cord
Three or more lesions in the periventricular white matter in the brain
At least one lesion in the infratentorial region, which includes the cerebellum
At least one lesion in the cortical or juxtacortical region of the brain – so in or near the grey matter
At least one lesion in an optic nerve
Preziosa emphasised that scoring cortical lesions (the grey matter) and lesions involving the white matter next to the cortex (called juxtacortical lesions) when assessing ‘dissemination in space’ was a key change to the current criteria and one that required detailed investigation within a clinical study.
The MAGNIMS study to test out the new criteria
During their work on the recent consensus statements, the MAGNIMS group set up a study involving 72 patients with CIS who were recruited from five European centres and followed up for over 2 years. One of the objectives was to reveal better the lesions present in the grey matter and in the adjacent white matter.
Finding lesions in or near the grey matter can be particularly difficult: Preziosa explained that patients in the study had a double inversion recovery MRI (DIR MRI) scan at study entry as this increases grey matter lesion detection compared to standard MRI.
After two years, 90% of those recruited to the study had developed MS, while 10% were found to have a separate neurological condition.
Encouragingly, the use of DIR MRI to detect lesions in the grey matter led to more patients being correctly diagnosed with MS right at the start of the study.
The group concludes that the changes that they have proposed to the diagnostic criteria for MS do indeed make it possible to diagnose MS in someone with very early clinical symptoms much more accurately.
These refinements in criteria seem to be small steps, but for patients with early stage MS, they are very significant. Being able to give someone an accurate diagnosis of MS enables disease-modifying treatments to be given as early as possible. Equally, if someone does not have MS, their clinical team can then move forward to finding out what is the cause of their symptoms.
Professor David Miller, Vice President & Chair of Scientific Committee of ECTRIMS
How optic nerve imaging can help monitor therapeutic effects in MS
Presentations revealed how imaging the retina and optic nerves can provide key information on disease progression in MS, including how effective treatment strategies are at slowing down those changes.
A comprehensive series of reviews, data and original reports explored and defined how researchers can use the visual system to better understand the disease process responsible for MS – including, how imaging of the optic nerve and retina can offer an interventional trial platform for proof of concept studies.
The importance of OCT imaging
Peter Calabresi (Director of the MS Center at Johns Hopkins, Baltimore, MD, USA), began the session by outlining the use and importance of Optical Coherence Tomography (OCT) as a non-invasive technique that is able to display and quantify retinal pathology. This standard imaging technology is widely available and is reproducible across different centers. In fact, it has been validated as a reliable indicator of disease progression in both longitudinal and cross-sectional datasets.
Using OCT to monitor drug response in MS
Raju Kapoor (University College, London, UK) described several clinical trials that have assessed the neuroprotective potential of various drugs by studying their effect on patients with optic neuritis. Using visual system imaging to monitor the impact of treatments on optic nerves themselves is a significant advance. However, more encouraging, is the potential of monitoring the response within the visual system could also provide information about the impact of the drug on lesions elsewhere in the central nervous system.
Can OCT scans predict disease progression?
In his introduction, Calabresi touched on a recent meta-analysis showing how well OCT retinal scans can accurately predict clinical outcomes five years later, mentioning an update on new data on predictions at 10 years. Alissa Rothman, a researcher in Calabresi’s group went into the study in more detail.
A total of 89 participants were included, most of them female patients with relapsing remitting MS who had a baseline expanded disability status scale (EDSS) of 2.8. Status OCT scans were performed on each patient at entry and follow up took place over a 10-year period. After using various models and adjusting for confounding factors such as age, sex and a history of optic neuritis, the total macular volume measured by the original OCT scans was found to accurately predict the EDSS scores at the ten-year follow up point.
In particular, the changes within the eye over the first 2-3 years seem to have the greatest predictive value.
Finally, Justin McKee (University of Oxford, UK) presented the results of the Amiloride Acute Optic Neuritis trial (the ACTION trial). Amiloride, a repurposed diuretic, which targets and blocks acid sensing ion channel 1 (ASIC1), is over-expressed in mouse models of MS and is present in post-mortem tissue from MS patients.
Previously, McKee explained, a cohort study in progressive MS had suggested that Amiloride may have a neuroprotective effect in MS. He then reported his group’s current study in which 48 patients with acute optic neuritis (within 28 days of onset) were given 10mg of Amiloride or a placebo. Treatment was continued for 5 months, then stopped for a month before outcomes were measured at 6 months and then again at 12 months.
Disappointingly, thickness of the retinal nerve fibre layer in the Amiloride treatment group was not significantly less than in the placebo group. The study included a number of secondary outcome measures, but no differences were observed between the groups here either.
Discussions following the presentation explored reasons for this negative result and many experts present focused on the therapeutic window in acute optic neuritis, which is very likely to be as little as 7 days. The potential of earlier treatment with Amiloride cannot be dismissed completely.
Research in this area of MS is now focusing on ways to understand the way in which immunomodulatory therapies work – we know they do, but we don’t understand fully how. Another major focus is to find out more about the mechanisms that lead to neuronal loss in MS so that we can develop new therapies to target MS progression that occurs without discernable inflammatory lesions.
Peter Calabresi, Director of the MS Center at Johns Hopkins, Baltimore, MD, USA
Lipoic acid shows great potential as a disease modifying treatment for secondary progressive MS
One of the parallel sessions reported promising early results on the potential benefits of lipoic acid in secondary progressive MS.
Lipoic acid is produced naturally in our own bodies and is found in many foods, and previous laboratory work has suggested that taking supplements of lipoic acid may help reduce some of the disabling effects of MS. Now this drug candidate is being tested in early stage human trial and can be added to the small number of drugs in development for secondary progressive MS.
Why could lipoic acid be so important?
Most people with MS initially have episodes of neurological symptoms that come and go. This stage of the disease is described as relapsing remitting MS and can last or months or even years. Eventually, however, most people develop deficits that progress over time and their disease is then termed secondary progressive MS.
Much of the progressive disability that occurs in secondary progressive MS is thought to be due to the loss of nerve cells and fibres. Treatments that could prevent or slow this loss could have the potential to prevent or slow disability progression.
Unfortunately, although we now have a range of treatments available for relapsing remitting MS, there are no licensed treatments for secondary progressive MS. As lipoic acid is inexpensive and readily available, and it is tolerated at high doses by MS patients, it is an attractive drug candidate.
Details of the lipoic acid study
In their double-blinded pilot treatment trial of lipoic acid, Chataway et al. studied 51 people with confirmed secondary progressive MS for 96 weeks.Lipoic acid, at a dose of 1200mg per day, was given to 27 patients, with a further 24 receiving a placebo. Participants were monitored using MRI scans to measure whole brain atrophy, atrophy of brain substructures and the spinal cord, atrophy of the retina and macular region in the eye, and by clinical assessment and questionnaires to determine impact on symptoms and quality of life.
At the end of the trial, MRI scans revealed a lower rate of whole brain atrophy in the lipoic acid treatment group compared to the placebo group. The rate of brain volume decline over time in those who took lipoic acid supplements was 0.22% per year and 0.65% per year in those who took the placebo. This is a 66% reduction, which is statically significant (p=0.004).
Lipoic acid treatments were well tolerated
The rate of serious adverse events was very similar between both groups. People in the lipoic acid group reported a higher rate of stomach upsets (an adverse effect) and a lower rate of falls (a benefit).
A very positive sign was also that more than 80% of the participants took the tablets regularly throughout the study period and only five participants withdrew during the course of the trial.
Taking lipoic acid forward in clinical trials
The study group recognises that this trial is a pilot. However, the strength of the response seen in patients with secondary progressive MS was sufficiently promising to warrant a larger trial to confirm the possible neuroprotective effects of lipoic acid and to further explore both the clinical benefits and the potential adverse effects.
The MS-STAT trial of high dose simvastatin has also shown a reduction in the rate of brain volume loss, and the EXPAND trial of siponimod, which will be presented at ECTRIMS tomorrow, has shown a beneficial effect on disability progression. Add in this study on lipoic acid and we are beginning to see several promising treatments emerge for secondary progressive MS.
Prof. Xavier Montalban, President of the European Committee for Treatment and Research In Multiple Sclerosis
Real world data from Biogen affirms efficacy of Tecfidera and 9 year safety profile
Further data show benefits of patient coaching in reducing discontinuation rates
Data presented from both real-world and clinical settings demonstrated that dimethyl fumarate delivered consistent1 and sustained efficacy2 among patients with relapsing-remitting multiple sclerosis (RRMS), and adds to its safety profile for up to nine years of treatment.3
Real world findings demonstrate efficacy of dimethyl fumarate versus other MS therapies
Retrospective results from the worldwide MSBase registry show that dimethyl fumarate reduced the risk of first relapse versus interferons by 26% (n=420 matched pairs; HR 0.74; 95% CI 0.57, 0.97; p=0.027), glatiramer acetate by 28% (n=382; 0.72; 0.54, 0.95; p=0.022) and teriflunomide by 34% (n=256; 0.66; 0.45, 0.99; p=0.042). In the primary analysis, no significant difference was found versus fingolimod-treated patients (n=415; 1.03; 0.73, 1.46; reference = FTY).1 Time to first relapse was measured using binomial propensity score matching.
The MSBase registry is one of the largest sources of real-world data and includes nearly 40,000 MS patients across 72 countries. Our analysis shows that dimethyl fumarate significantly reduced the risk of first relapse compared to platform therapies and teriflunomide, and had comparable efficacy to fingolimod
H. Butzkueven, Associate Professor in the Department of Medicine, University of Melbourne and one of the investigators for the study
As a secondary endpoint, the study also demonstrated similar and consistently lower annualised relapse rates (ARR) for dimethyl fumarate-treated patients versus those treated with interferons (0.23 [95% CI 0.19, 0.27] vs 0.26 [0.24, 0.29]), glatiramer acetate (0.24 [0.19, 0.28] vs 0.26 [0.23, 0.29]) and teriflunomide (0.17 [0.13, 0.22] vs 0.27 [0.22, 0.33]). ARR for dimethyl fumarate-treated patients was found to be similar but higher versus fingolimod-treated patients (0.22 [0.18, 0.27] vs 0.19 [0.17, 0.23]).1
Positive ARR findings were also reported in a second real-world study analysing data from over 3,500 dimethyl fumarate-treated patients from a US Commercial Claims Database. An average reduction in ARR of -0.11 (0.41 vs 0.30; p<0.05) was demonstrated in the year following initiation of dimethyl fumarate versus the year before initiation.4
The MSBase registry data also found that approximately twice as many dimethyl fumarate-treated patients discontinued treatment after six months of continuous therapy relative to fingolimod (HR 2.39; 95% CI 1.78, 3.20) and interferons (HR 1.40; 95% CI 1.07, 1.83).1 No difference was found versus glatiramer acetate (HR 1.18; 95% CI 0.89, 1.56) or teriflunomide (HR 0.95; 95% CI 0.66, 1.37).1
The use of patient coaching to reduce discontinuation rates was demonstrated in a retrospective real-world study. In patients treated with dimethyl fumarate, rates were reduced in coached patients by up to 48% versus controls (5.7%, 17.1% and 29.2% of coached patients [n=4750] stopped therapy after 3, 12 and 24 months, versus 10.4%, 25.2% and 56.4% of controls [n=3266], respectively).5
Reasons for therapy discontinuation differed between coached and control patients, with partly manageable side effects found to be the main reason for discontinuation for controls. These results could indicate the potential for patient coaching to play an essential role in overcoming such side effects for dimethyl fumarate patients.5
Additional real-world data presented by Biogen demonstrated that the safety profile of dimethyl fumarate remained consistent over nine years,3 and its overall benefit-risk remained favourable.6 These data also further substantiate current guidance for monitoring absolute lymphocyte counts (ALC) to mitigate the risk of moderate to severe prolonged lymphopenia during treatment with dimethyl fumarate.6
Data from ENDORSE further clarify benefits of dimethyl fumarate for newly-diagnosed patients
New 7-year data from the ENDORSE study, an extension to the DEFINE and CONFIRM clinical trials, demonstrated that ARR remained low at 7 years for both treatment groups (0.13 [95% CI 0.10–0.18] with dimethyl fumarate; 0.16 [95% CI 0.11–0.24] for patients switched from placebo). Switch patients experienced a 61% relative reduction in ARR following the switch to dimethyl fumarate after 2 years on placebo (ARR 0.26 [95% CI 0.18–0.37] vs 0.10 [0.07–0.15]; p<0.0001).2 These findings illustrate the potential of dimethyl fumarate to provide positive clinical outcomes over the long-term for people with relapsing remitting MS.
In addition, estimated 24-week confirmed disability progression (CDP) was 18.0% (95% CI 12.0–26.4) in the dimethyl fumarate group versus 26.4% (95% CI 17.4–38.7) in the switch group, representing a 41% risk reduction (95% CI 0.32–1.10, p=0.0979).2
References:
Spelman T, et al.Comparative analysis of MS outcomes in dimethyl fumarate-treated patients relative to propensity matched fingolimod, interferon, glatiramer acetate, or teriflunomide. P1157. The 32ndCongress of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS), London, England, 14–19 September 2016.
Gold R, et al.Seven-year follow-up of the efficacy of delayed-release dimethyl fumarate in newly diagnosed patients with relapsing-remitting multiple sclerosis: integrated analysis of DEFINE, CONFIRM, and ENDORSE. P631. The 32ndCongress of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS), London, England, 14–19 September 2016.
Fox RJ, et al.Absolute lymphocyte count and lymphocyte subset profiles during long-term treatment with delayed-release dimethyl fumarate in patients with relapsing-remitting multiple sclerosis. P716. The 32ndCongress of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS), London, England, 14–19 September 2016.
Boster A, et al.Annual relapse rates in multiple sclerosis patients treated with different disease-modify therapies – findings from a real world setting. EP1481. The 32ndCongress of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS), London, England, 14–19 September 2016.
Begus-Nahrmann Y, et al.The potential of individualized patient coaching to optimize treatment with delayed-release dimethyl fumarate: a retrospective analysis of patients with multiple sclerosis treated in a real-world setting. P1214. The 32ndCongress of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS), London, England, 14–19 September 2016.
Buckle G, et al.Effect of delayed-release dimethyl fumarate on lymphocyte subsets in patients with relapsing multiple sclerosis: a retrospective, multicentre, observational study (REALIZE). EP1495. The 32ndCongress of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS), London, England, 14–19 September 2016.
Sign up to receive our email newsletter with links to the latest content. ACNR is free, thanks to the support of advertisers. The editorial content is peer reviewed and remains completely independent unless clearly specified.